History and exam
Key diagnostic factors
common
sudden-onset (<72 hours) unilateral facial weakness
Sudden-onset (<72 hours) unilateral peripheral facial weakness can be partial or complete, and is present in around 90% of patients with Ramsay Hunt syndrome.[6][9][12] It often presents with severe ear/facial pain, vesicular rash (including blisters), hearing loss, and/or vertigo.
[Figure caption and citation for the preceding image starts]: Right facial palsy in a man with Ramsay Hunt syndrome. Note the inability to close the right eye (A) and significant smile asymmetry (B), both frequently seen in acute Ramsay Hunt syndromeFrom the collection of Dr Matthew Miller; used with permission [Citation ends].
However, patients do not always present with the classic triad of unilateral facial paralysis, severe ear/facial pain, and vesicular ear rash. Consider other causes of sudden-onset facial paralysis such as Bell’s palsy, cerebrovascular accident, and Lyme disease when evaluating these patients.
ipsilateral severe ear/facial pain
Patients present with pain around one ear and face on the same side of facial weakness.[6][9][12] The pain is typically severe.[6]
However, patients do not always present with the classic triad of facial paralysis, severe ear/facial pain, and vesicular ear rash. Consider other causes of sudden-onset facial paralysis such as Bell’s palsy, cerebrovascular accident, and Lyme disease when evaluating these patients.
ipsilateral vesicular rash
The presence of vesicles in the external ear and auditory canal is highly suggestive of varicella zoster virus (VZV) reactivation in Ramsay Hunt syndrome. The vesicles, including blisters, can precede, coexist with, or follow facial palsy. The vesicles may be seen on the external ear alone (around 41% of patients) or on both the external ear and external ear canal (around 25% of patients).[12] They may be associated with pain affecting the outer portion of the pinna and outer third of the external ear canal.[6] Some patients may present solely with redness of the skin in the ear canal and ear drum. [Figure caption and citation for the preceding image starts]: Painful vesicular rash in ear in a patient with Ramsay Hunt syndromeFrom the collection of Dr Matthew Miller; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: External acoustic meatus with multiple vesicular lesions in a patient with Ramsay Hunt syndromeAyoub F et al. BMJ Case Rep. 2017 Jul 13;2017:bcr20172198366; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: External acoustic meatus with multiple vesicular lesions in a patient with Ramsay Hunt syndromeAyoub F et al. BMJ Case Rep. 2017 Jul 13;2017:bcr20172198366; used with permission [Citation ends].
However, patients do not always present with the classic triad of facial paralysis, severe ear/facial pain, and vesicular ear rash. Consider other causes of sudden-onset facial paralysis such as Bell’s palsy, cerebrovascular accident, and Lyme disease when evaluating these patients.
absence of constitutional symptoms
Fever, general malaise, myalgia, arthralgia, headache, or rash (erythema migrans or other) suggest an alternative diagnosis, such as Lyme disease, autoimmune disorder, or granulomatous disease.
Other diagnostic factors
common
dry eye
May occur due to the inability to close the eye on the affected side.[6]
vertigo
A common otologic symptom.[9]
hearing loss
A common otologic symptom.[9]
tinnitus
A common otologic symptom.[9]
epiphora
A common ocular symptom.[9]
altered taste
A common symptom.[9]
oral lesions
A common symptom.[9]
Vesicles, including blisters, are most commonly seen on the ear but may also be present on the cheek, tongue, and palate.[6]
[Figure caption and citation for the preceding image starts]: A) Vesicular rash on the tongue and B) the palate in a patient with Ramsay Hunt syndromeNeagu MR et al. Pract Neurol. 2016 Jun;16(3):232; used with permission [Citation ends].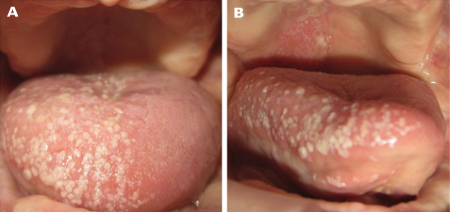
uncommon
keratitis
Patients with ocular symptoms, especially if there is significant involvement in the V1 and V2 dermatomes in addition to facial weakness, are at risk for corneal injury. This is due to the patient's inability to close the eye. Keratitis may develop in these patients.[6]
Risk factors
strong
prior exposure to varicella zoster virus (VZV)
The pathophysiology of Ramsay Hunt syndrome involves reactivation of varicella zoster virus (VZV), where it generally lies dormant in the geniculate ganglion (CN VII) or sensory ganglion of the face (CN V).[7] Although it has been reported that people without prior VZV vaccination or known infection have been diagnosed with Ramsay Hunt syndrome, this is uncommon (0.5% to 1.0% of patients with herpes zoster reported no prior vaccination or known infection in one small population-based study of people ages <20 years).[8]
age >50 years
The pathophysiology underlying Ramsay Hunt syndrome is likely due to adaptive immunity declining as patients age. VZV infections often occur in childhood, and vaccinations have been widely available since the mid-1990s for school-aged children. For example, in the US, herd immunity to VZV due to the successful widespread vaccination campaign means that most people's immune systems have not been exposed to VZV since childhood. Therefore, the waning of adaptive immunity is responsible for the increased prevalence of VZV reactivation in patients ages over 50 years, reaching 50% by 85 years.[5]
immunosuppression
People who are immunosuppressed are more susceptible to VZV infection and are at higher risk of developing more severe disease and having less chance of a complete recovery.[6]
weak
recent physiological stressor
female sex
There appears to be a slightly higher incidence of Ramsay Hunt syndrome in females than in males. The specific mechanism for this is not clearly understood.
Use of this content is subject to our disclaimer