Etiology
The etiology of ovarian cancer is poorly understood.
Inherited genetic mutations in BRCA1 or BRCA2 represent a significant risk factor for ovarian cancer.[10][11][12][13] Ovarian cancer associated with BRCA mutations is usually high-grade and predominantly serous or endometrioid.[13]
An increased risk of ovarian cancer (and other gynecologic cancers) is also found in patients with Lynch syndrome (formerly referred to as hereditary nonpolyposis colorectal cancer), a rare hereditary condition involving mutations of DNA mismatch repair genes (including MSH2, MLH1, MSH6, and PMS2) and deletions in the EPCAM gene.[14][15]
Other gene mutations associated with hereditary ovarian cancer (as well as breast and other cancers) include ATM, BRIP1, NBN, PALB2, STK11, RAD51C, and RAD51D.[16][17][18]
Studies of prophylactic salpingo-oophorectomy in women with BRCA mutations have revealed that many early cancers in these women arise in the fallopian tube, and that the distal fimbrial portion is the most common site of origin.[4][19][20][21][22][23] Additionally, serous tubal intraepithelial carcinoma (STIC) has been identified as a precursor lesion for high-grade serous ovarian carcinoma, the most common type of epithelial ovarian cancer.[4][19][22][23]
Pathophysiology
Epithelial ovarian cancer does not typically invade into organ space parenchyma, but instead attaches to the surface of organs. Tumor cells implant along the lining of the peritoneal cavity (local advancement), bowel mesentery, and liver capsule, indicating metastatic disease. Malignant transformation may be related to tumor suppressor gene mutations (e.g., BRCA and TP53) for high-grade tumors, and mutations of proto-oncogenes (e.g., BRAF and KRas) for low-grade tumors.[24][25][26][27]
Exfoliated cancer cells follow the natural circulation of the peritoneal fluid, along the right paracolic gutter and subdiaphragmatic space. Thus, the right liver edge and diaphragm peritoneum are common sites of tumor implantation. The omentum also is a common site of tumor implantation.[Figure caption and citation for the preceding image starts]: Omentum infiltrated with tumorFrom the collection of Justin C. Chura, MD, Cancer Treatment Centers of America, Philadelphia, PA [Citation ends].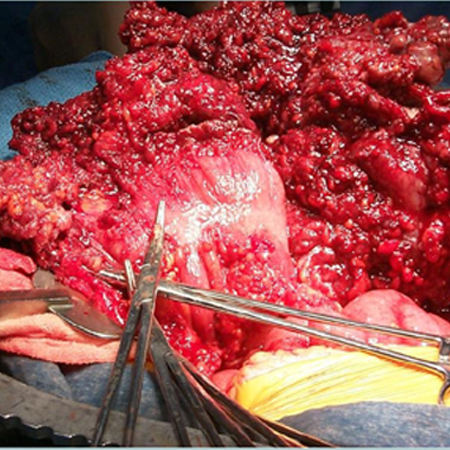 The initial spread pattern of ovarian cancer is by direct spread or lymphatic drainage. Hematogenous dissemination typically occurs late in the disease process.[28]
The initial spread pattern of ovarian cancer is by direct spread or lymphatic drainage. Hematogenous dissemination typically occurs late in the disease process.[28]
Classification
World Health Organization (WHO) classification of female genital tumors (2020)[5]
Epithelial ovarian tumors are classified by cell type (e.g., serous, endometrioid, mucinous, clear cell, Brenner, or seromucinous) and atypia (e.g., malignant, borderline, or benign).
Serous tumors
Malignant
Low-grade serous carcinoma
High-grade serous carcinoma
Carcinoma in situ and grade III intraepithelial neoplasia
Serous carcinoma, noninvasive, low-grade
Serous borderline tumor, micropapillary variant
Borderline
Serous borderline tumor
Benign
Serous cystadenoma
Serous surface papilloma
Serous adenofibroma
Serous cystadenofibroma
Endometrioid tumors
Malignant
Endometrioid adenocarcinoma
Seromucinous carcinoma
Borderline
Endometrioid borderline tumor
Benign
Endometrioid cystadenoma
Endometrioid adenofibroma
Mucinous tumors
Malignant
Mucinous adenocarcinoma
Borderline
Mucinous borderline tumor
Benign
Mucinous cystadenoma
Mucinous adenofibroma
Clear cell tumors
Malignant
Clear cell adenocarcinoma
Borderline
Clear cell borderline tumor
Benign
Clear cell cystadenoma
Clear cell adenofibroma
Brenner tumors
Malignant
Malignant Brenner tumor
Borderline
Borderline Brenner tumor
Benign
Brenner tumor
Seromucinous tumors
Borderline
Seromucinous borderline tumor
Benign
Seromucinous cystadenoma
Seromucinous adenofibroma
Use of this content is subject to our disclaimer