Differentials
Lymphoma
SIGNS / SYMPTOMS
History of persistently enlarged lymph nodes, constitutional or B symptoms (fevers, night sweats, and/or weight loss). Usually under age 35 or over age 65. Physical exam may reveal lymphadenopathy in one or more regions; hepatosplenomegaly may be present.
If there is involvement of the anterior mediastinum alone, it may be difficult to differentiate lymphoma from thymic malignancy radiographically.
INVESTIGATIONS
Chest CT scan usually shows a more multinodular, aggressive, or invasive mass, but not always. If there is peripheral lymphadenopathy, excision biopsies will reveal the type of lymphoma. If lymphoma involves the anterior mediastinum alone, core needle biopsy will be required to differentiate from thymic malignancy.
Malignant mediastinal germ cell tumor: seminoma
SIGNS / SYMPTOMS
Occurs in people aged 20 to 40 years, with male predominance.
Presenting symptoms depend on tumor location, growth rate, and size; they include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea.
INVESTIGATIONS
Chest CT scan usually shows homogeneous invasive malignant-appearing anterior mediastinal mass.
Serum alpha-fetoprotein normal; may have low-level elevation of serum human chorionic gonadotropin (beta-hCG).
Malignant mediastinal germ cell tumor: nonseminoma
SIGNS / SYMPTOMS
Patient is typically a young male with significant symptoms of systemic and local invasion, such as fatigue, weight loss, fever, dyspnea, and chest pain.
INVESTIGATIONS
Serum alpha-fetoprotein and human chorionic gonadotropin (beta-hCG) usually elevated.
Chest CT scan usually shows a large inhomogeneous invasive mass with areas of hemorrhage and necrosis; pleural effusion often present; may show lung metastases.
Benign mediastinal germ cell tumor
SIGNS / SYMPTOMS
Typically asymptomatic because of slow growth rate of the tumor.
If present, the most common symptoms are dyspnea and substernal chest pain.
INVESTIGATIONS
On chest CT, mature (low-grade) teratoma has a pathognomonic CT appearance with cystic, fatty, and/or calcified components.
Substernal goiter
SIGNS / SYMPTOMS
Older patient usually without symptoms. Rarely, patients have upper-chest discomfort, dyspnea, or hoarseness. Symptoms of hyperthyroidism (heat intolerance, weight loss) or hypothyroidism may be present.
A visible goiter is present in 80% to 90% of patients; substernal extension is suggested if the lower pole of the thyroid gland cannot be identified. Airway compression may present with stridor and prolonged inspiration/expiration. Signs of thyrotoxicosis, including weight loss, hypertension, and tachycardia, may be evident on physical exam. Tracheal deviation can occur if the goiter is asymmetric. Pemberton signs (neck vein distension and facial flushing when arms are held vertically above head [Pemberton maneuver]) may be present.
INVESTIGATIONS
Chest CT shows anterior mediastinal mass nearly always contiguous with the thyroid, and tending to also involve the middle mediastinum/paratracheal space; mass often has low-density areas and calcifications; if goiter is suspected, iodinated contrast should be avoided (due to risk of iodine-induced hypothyroidism; Jod-Baselow effect).
Thyroid function tests may be abnormal.
Thymic hyperplasia
SIGNS / SYMPTOMS
Usually asymptomatic, but can be seen with myasthenia gravis, Graves disease, burns, after viral illnesses, and as a rebound phenomenon (e.g., after chemotherapy or corticosteroid therapy, especially for Hodgkin disease).
INVESTIGATIONS
Chest CT usually shows enlargement of the typical shape of the thymus (bilobed) without a dominant or discrete rounded mass. [Figure caption and citation for the preceding image starts]: CT scan of the chest showing a prominent thymic gland with bilobed appearance, consistent with thymic hyperplasiaFrom the collection of Cameron Wright, MD; used with permission [Citation ends].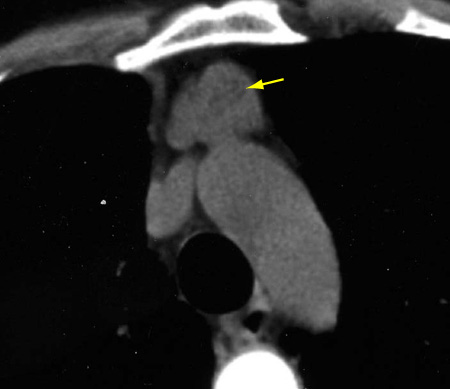
Chemical-shift MRI may be helpful in differentiating hyperplasia from tumor in problematic cases.
Thymic cyst
SIGNS / SYMPTOMS
Usually asymptomatic and an incidental finding. Some cysts can be large and heterogenous on imaging.
INVESTIGATIONS
MRI is helpful to distinguish between a cyst and solid tumor. No fluorine-18 fluorodeoxyglucose-avidity with PET scans.
Use of this content is subject to our disclaimer