Differentials
Measles (rubeola)
SIGNS / SYMPTOMS
Measles is a more severe illness. Erythematous or brownish morbilliform rash spreads from the head and neck downward and persists for 3 to 7 days. Coryza, cough, and conjunctivitis are usual.
A pathognomonic enanthem (Koplik spots) occurs early in the disease. Complications are common, particularly in immunocompromised and malnourished people.[Figure caption and citation for the preceding image starts]: Koplik spotsCDC Public Health Image Library [Citation ends].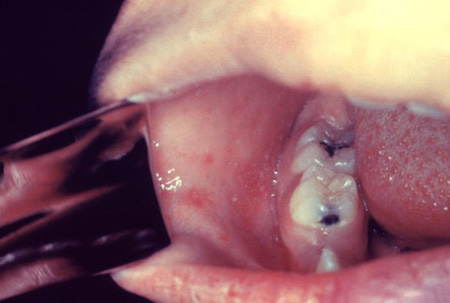 [Figure caption and citation for the preceding image starts]: Child with measles showing the characteristic red blotchy rash on his buttocks and back during the third day of the rashCDC Public Health Image Library [Citation ends].
[Figure caption and citation for the preceding image starts]: Child with measles showing the characteristic red blotchy rash on his buttocks and back during the third day of the rashCDC Public Health Image Library [Citation ends].
INVESTIGATIONS
Positive serum measles anti-IgM antibody is the preferred test (sensitivity 83% to 89%, specificity 87% to 100%).[25][26]
Significant rise in serum measles anti-IgG antibody in paired acute and convalescent specimens.
Isolation of measles virus from throat, nasopharynx, blood, or urine (usually processed by public health and reference laboratories only).
Roseola infantum (HHV-6, HHV-7, exanthem subitum, sixth disease)
SIGNS / SYMPTOMS
Typically affects children <2 years of age.[27] Coryza, conjunctivitis, and cervical or occipital lymphadenopathy may precede 3 to 7 days of high fever and irritability. Development of an erythematous or pinkish maculopapular rash coincides with the resolution of fever and persists for hours to several days. Febrile seizures occur in 10% to 15%.
INVESTIGATIONS
Anti-HHV-6/HHV-7 IgG antibody seroconversion between paired acute and convalescent specimens is the preferred test.[28] Increases in serum-specific antibody occur with viral reactivation. Specific serum IgM testing is not reliable. HHV-6 and HHV-7 are serologically cross-reactive.
Positive HHV-6/HHV-7 nucleic acid amplification from serum or plasma (sensitivity 90% to 100%, specificity 100%). Cannot distinguish acute infection from reactivation.[29]
Isolation of virus from peripheral blood (usually processed by public health and reference laboratories only).
Scarlet fever (group A Streptococcus pyogenes)
SIGNS / SYMPTOMS
Most common in school-age children. Usually associated with streptococcal pharyngitis, but occasionally complicates skin and soft-tissue infection.
Pharyngitis, anterior cervical adenopathy, and fever precede a confluent erythematous blanching "sandpaper" rash that begins on the trunk and behind the ears and is accentuated in flexural creases. Rash resolves with desquamation in 3 to 8 days.
Other features include an erythematous-coated "strawberry" tongue, circumoral pallor, and Pastia lines (linear erythematous lesions in skinfolds, particularly elbows and axillae). [Figure caption and citation for the preceding image starts]: The scarlet fever rash first appears as tiny red bumps on the chest and abdomen that may spread all over the body; looking like sunburn, it feels like a rough piece of sandpaper, and lasts about 2 to 5 daysCDC Public Health Image Library [Citation ends].
INVESTIGATIONS
Group A streptococcal rapid antigen testing is 60% to 85% sensitive and 90% to 100% specific.[30] Negative results should be confirmed by throat culture.
Isolation of group A streptococcus from throat culture on blood agar is 80% to 98% sensitive and 100% specific.
Erythema infectiosum (parvovirus B19, fifth disease)
SIGNS / SYMPTOMS
Most common in children. Mild systemic symptoms and/or fever are followed in 7 to 10 days by a distinctive erythematous facial rash with a "slapped cheek" appearance.
An erythematous lacy maculopapular rash may also appear on the trunk and spread peripherally to the arms and thighs. Occasionally the rash may be atypical and indistinguishable from that of rubella. Arthralgias and arthritis are more common with increasing age.
Enteroviral infections (echovirus, coxsackievirus)
SIGNS / SYMPTOMS
Incidence is highest in infants and young children and in the summer and early fall. Most common presentation is a nonspecific febrile illness. Neurologic and GI symptoms and stomatitis may be prominent.
INVESTIGATIONS
Nucleic acid amplification of enteroviral RNA from blood or CSF is the most rapid and sensitive test.[33]
Isolation of enterovirus from stool, rectal swabs, throat, blood, CSF, or urine.
Sensitivity and specificity vary, depending on the type of virus, site of infection, and time at which specimens are obtained.
West Nile virus
SIGNS / SYMPTOMS
Incidence highest in summer, coinciding with mosquito activity. Fever is generally higher than that observed with rubella, and headache, myalgias, and weakness are more prominent.
A diffuse erythematous maculopapular or morbilliform rash, which spares the palms and soles, is more common in children than adults. Neuroinvasive disease occurs in 0.3% to 1.0% of patients.
INVESTIGATIONS
Specific IgM by antibody capture ELISA are >95% sensitive and 83% to 99% specific after the first week of illness, but may persist for >1 year.[34]
Fourfold increase in virus-specific serum antibody titers. Cross-reactivity with other arboviruses may occur. Positive results should be confirmed by virus-specific IgG.
Isolation of virus from CSF or serum.
Virus-specific IgM in CSF or amplification of viral nucleic acid from CSF (neuroinvasive disease).
Dengue virus
SIGNS / SYMPTOMS
Dengue virus is a flavivirus that is transmitted to humans through the bite of Aedes mosquitos, blood transfusion, organ transplantation, occupational exposure to infected blood, or by in utero or perinatal infection.[35]
Dengue is endemic in many countries in Asia, the Pacific, Africa, the Caribbean, and the Americas, including Puerto Rico, the US Virgin Islands, Samoa, and Guam. Sporadic outbreaks have been reported in Florida, Hawaii, and the Texas-Mexico border, but most cases in the United States are acquired in endemic regions by travelers or immigrants.
Symptomatic patients with mild disease (dengue fever) may present with fever, severe headache, myalgias, arthralgias, and a diffuse erythematous maculopapular rash. Retro-orbital pain and mild hemorrhagic signs are common. More severe forms of disease are characterized by bleeding and shock due to plasma leak and intravascular volume depletion.
INVESTIGATIONS
Nucleic acid amplification of dengue virus RNA from serum, plasma, CSF, or tissue specimens is the most rapid and sensitive test in the first week of illness.
Most patients have serum anti-dengue IgM antibodies detectable by ELISA assay by the fifth day of illness. These may remain detectable for 2 to 3 months. IgG antibodies increase more slowly and remain elevated for months to years; comparison of acute and convalescent (with at least 7 days between samples) is useful in differentiating acute from distant infections.
Chikungunya virus
SIGNS / SYMPTOMS
Chikungunya virus is an alphavirus that is transmitted through the bite of Aedes mosquitos and, rarely, by perinatal infection.[36]
Most patients present with fever and severe joint pain. Headache, myalgias, arthritis, conjunctivitis, or a maculopapular rash may occur. Disease may be more severe in neonates, the elderly, and people with underlying medical conditions. Joint pain or arthritis may persist or recur over months to years.
Chikungunya virus outbreaks have been reported in many countries in Africa, Asia, Europe, the Pacific, the Caribbean, and South America. In the US, most infections have been reported in travelers returning from these areas. Locally-transmitted infections have been reported in Florida, Texas, Puerto Rico and the US Virgin Islands.
INVESTIGATIONS
Nucleic acid amplification of chikungunya virus RNA from serum or plasma is the most rapid and sensitive test in the first week of illness.
Specific anti-chikungunya IgM and neutralizing antibodies may be detectable towards the end of the first week of illness. Comparison of acute and convalescent sera is recommended.
Zika virus
SIGNS / SYMPTOMS
Zika virus is a flavivirus that is transmitted to humans through the bite of Aedes mosquitoes, by sexual contact with people infected with Zika virus, blood transfusion, or by in utero or perinatal infection.[37]
Zika virus infection should be suspected in returned travelers from endemic areas or those with other epidemiologic risk factors.
Zika virus outbreaks have been reported in many tropical and subtropical regions of the world. Local mosquito-borne transmission has been reported in Puerto Rico, the US Virgin Islands, and American Samoa. There have been no confirmed cases, however, reported from the continental US or US territories since 2019.[38] Most people with Zika virus infection are asymptomatic. Features of symptomatic disease include fever, a maculopapular rash, arthralgia, myalgia, headache, and conjunctivitis. Symptoms are generally mild and persist for days to a week. Rare complications include Guillain-Barre syndrome. Complications of Zika virus infection in pregnant women include fetal loss, microcephaly, and congenital central nervous system and ocular abnormalities.
INVESTIGATIONS
Currently, Zika virus testing can be obtained through commercial laboratories, the CDC Arboviral Diagnostic Laboratory and several state health departments.[39]
Zika virus can be tested for by PCR during the first week after disease onset. Specific IgM and neutralizing antibodies begin to develop late in the first week of illness. Cross-reactions with other flaviviruses are common, so positive, equivocal, or inconclusive tests should be confirmed by plaque-reduction neutralization assay.
Secondary syphilis
SIGNS / SYMPTOMS
A generalized polymorphous maculopapular rash begins on the trunk and typically involves the palms and soles. Other common manifestations include condyloma lata, mucosal lesions, and generalized lymphadenopathy.
Fever and other constitutional symptoms are not prominent. Clinical manifestations resolve spontaneously or with treatment over several weeks to months. [Figure caption and citation for the preceding image starts]: Patient with a syphilitic roseola-like rash, similar to that of viral eczema, which developed on her buttocks and legs during the secondary stage of the diseaseCDC Public Health Image Library; from the collection of J. Pledger, BSS/VD; used with permission [Citation ends].
INVESTIGATIONS
Positive VDRL, RPR tests are 100% sensitive and 93% to 99% specific.[40]
Results should be confirmed by a specific treponemal test (FTA-ABS, 100% sensitive and 94% to 100% specific).
Identification of spirochetes by dark-field exam of scrapings from moist mucocutaneous lesions.
Infectious mononucleosis (Epstein-Barr virus)
SIGNS / SYMPTOMS
High fever, exudative pharyngitis, cervical or generalized lymphadenopathy, hepatosplenomegaly, and an atypical lymphocytosis are common in adolescents and adults.
Periorbital edema is frequently observed early in infection. Children are more likely to be asymptomatic or have a mild form of illness. A polymorphous rash, usually on the trunk and arms, occurs in up to 20% of cases. Rash is more common in patients treated with ampicillin and other penicillins. Sometimes conjunctival hemorrhage may be seen. [Figure caption and citation for the preceding image starts]: A conjunctival hemorrhage of the right eye of this patient with infectious mononucleosisCDC Public Health Image Library; from the collection of Thomas F. Sellers, Emory University; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Tongue and palate of patient with infectious mononucleosisCDC Public Health Image Library; from the collection of Dr Sellers, Emory University; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Tongue and palate of patient with infectious mononucleosisCDC Public Health Image Library; from the collection of Dr Sellers, Emory University; used with permission [Citation ends].
INVESTIGATIONS
Positive anti-viral capsid antigen (VCA) IgM antibodies are detectable in the second week of illness and disappear over several months. Anti-VCA IgG antibody is also detectable early in infection and persists for life, whereas anti-EBV-associated nuclear antigen (EBNA) antibody develops weeks to months after infection. The presence of anti-VCA Ab and absence of anti-EBNA Ab are diagnostic of acute infection (sensitivity 95% to 100%, specificity 86% to 100%).[41]
Heterophile antibody testing (monospot) is sensitive (81% to 95%) and specific (98% to 100%) in school-age children and adults, but is insensitive in young children.
Kawasaki syndrome
SIGNS / SYMPTOMS
Occurs almost exclusively in children <8 years of age. Prominent features are a persistent high fever, bulbar conjunctivitis, erythematous changes of the mouth and pharynx, and dry, cracked lips, swelling and pain of the hands and feet, and cervical lymphadenopathy.
Irritability, abdominal pain, diarrhea, and vomiting are common. Periungual desquamation may be noted in the second week of the illness. Coronary and other arterial aneurysms may develop 1 to 4 weeks after the onset of illness.
INVESTIGATIONS
No specific diagnostic test is available.
Suggestive laboratory and diagnostic imaging findings include sterile pyuria, hepatitis, CSF pleocytosis, pericardial effusion, gallbladder hydrops, and coronary artery abnormalities.
Cutaneous drug reaction
SIGNS / SYMPTOMS
Medications commonly associated with cutaneous reactions include antibiotics and anticonvulsants. Many drug-induced rashes have characteristic features (erythema multiforme, urticaria). [Figure caption and citation for the preceding image starts]: Bullous erythema multiformeCDC Public Health Image Library; from the collection of Dr John Noble, Jr; used with permission [Citation ends].
INVESTIGATIONS
Clinical diagnosis based on exposure history, resolution after withdrawal of the implicated drug, and exclusion of other potential causes. Eosinophilia is suggestive, but not diagnostic, of cutaneous drug reactions.
Juvenile rheumatoid arthritis
SIGNS / SYMPTOMS
Systemic-onset juvenile rheumatoid arthritis commonly affects children and adolescents. Children are often ill-looking. Typically there are daily high-spiking fevers that, in the absence of therapy, persist for weeks to months.
The rash is evanescent, salmon-colored, and linear and typically involves the trunk and extremities. The presence of the rash often coincides with fever. Mild hepatosplenomegaly and myalgias (or muscle tenderness) are common. Serositis may occur.
Many patients develop a chronic synovitis of ≥1 joints, but the onset of joint involvement may be delayed.
INVESTIGATIONS
There is no definitive laboratory test. Leukocytosis, thrombocytosis, anemia, elevated ESR, and elevated serum ferritin concentrations are suggestive.
Use of this content is subject to our disclaimer