Approach
IgAV is usually diagnosed clinically, based on characteristic features in the history and physical exam. The combination of a purpuric rash, combined with polyarthralgias, abdominal pain, and renal disease, is indicative of the disease.[1]
Diagnosis is more difficult in patients with an unusual presentation, such as the rare findings of pulmonary hemorrhage, headaches, or seizures, followed by the development of a rash. It may be made only after biopsy of an affected organ (such as skin or kidney), which shows IgA deposition.
This section focuses on the diagnosis of children only. Discussion of the diagnosis in adults is beyond the scope of this topic.
Diagnostic criteria
The presence of two or more of the 1990 American College of Rheumatology criteria (i.e., palpable purpura, age at onset <20 years, abdominal pain, or wall granulocytes on biopsy) has a sensitivity of 87.1% and a specificity of 87.7%.[28]
Consensus recommendations published in 2019 by the European SHARE initiative (Single Hub and Access point for paediatric Rheumatology in Europe) endorse the EULAR/PRINTO/PRES (European League Against Rheumatism; Paediatric Rheumatology International Trials Organisation; Paediatric Rheumatology European Society) criteria for clinical diagnosis.[29][30] EULAR/PRINTO/PRES criteria require the presence of purpura or petechiae (mandatory) with lower limb predominance and at least one of the four following criteria:[30]
Abdominal pain
Histopathology
Arthritis or arthralgia
Renal involvement.
History
History typically reveals the development of a rash, arthralgias, and abdominal pain. Exploration of aggravating factors may reveal symptoms occurred following an upper respiratory tract infection, gastrointestinal (GI) upset, history of recurrent tonsillitis, or drug ingestion (a full drug history should be taken).
Uncommon but important symptoms may include testicular swelling or pain, headaches, hemoptysis, or seizures.[9][10]
Physical exam
Skin lesions are characterized as palpable purpura, and are typically non-blanching. They can occur anywhere on the body, but they are usually concentrated on the lower leg extending up to the buttocks. Rash on the trunk or face is uncommon.
Polyarthralgia can be present and is often associated with edema and abdominal pain on examination. Scrotal pain and swelling may occur in boys.[9] Neurologic examination will rarely reveal focal deficits. Pulmonary hemorrhage is a rare presentation.[Figure caption and citation for the preceding image starts]: Palpable purpura on the lower extremities of a childFrom the collection of Paul F. Roberts, MD [Citation ends].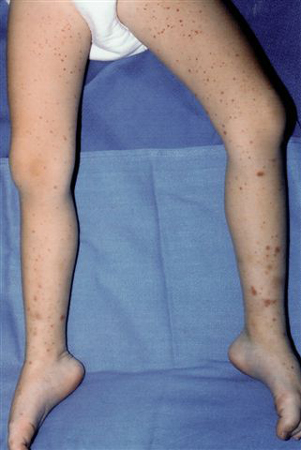
Laboratory evaluation
Renal involvement should be investigated by tests including blood pressure measurement, early morning urinalysis (to determine presence of hematuria and quantify urine protein:creatinine ratio), and assessment of renal function using estimated glomerular filtration rate (eGFR). Urinalysis should be monitored in all patients for at least 6 months after diagnosis.[31]
A pediatric nephrologist should be consulted if a patient with IgAV has moderate proteinuria and/or impaired GFR to discuss whether a renal biopsy is required.[29]
Serum IgA levels may be elevated, but this is not a specific test for IgAV and is not routinely performed.
A complete blood count and coagulation studies will help to exclude other causes, and a septic (infection) screen is warranted if the rash presents with fever.
Antinuclear antibodies, antineutrophil cytoplasmic antibodies, and complement levels will help to differentiate IgAV from other vasculitides.

How to take a venous blood sample from the antecubital fossa using a vacuum needle.
Skin biopsy
A skin biopsy, including specific staining for IgA, should be performed in cases of atypical rash (such as extensive lesions or diffusely distributed lesions). Skin biopsy excludes alternative diagnoses including other forms of vasculitis, such as ANCA-associated vasculitis, particularly in older children.[29]
Skin biopsies should be of the most recent lesions. The absence of IgA staining on biopsy does not exclude the diagnosis of IgAV.
Renal biopsy
A renal biopsy should be performed if a patient with IgAV has:[29]
Severe proteinuria (>250 mg/mmol at least 4 weeks after diagnosis; shorter duration of severe proteinuria is a relative indication for biopsy)
Persistent moderate proteinuria, or
Persistent impaired GFR.
Additional indications for renal biopsy include:[29]
Acute kidney injury with worsening renal function
Patients who are nephrotic (e.g., heavy proteinuria, hypoalbuminemia, and edema) or nephritic (e.g., impaired eGFR, hypertension, hematuria/proteinuria) at any time point.
The UK Kidney Association guideline on IgAV in children and young people recommends classifying kidney histology using the International Study of Kidney Disease in Children (ISKDC) classification criteria.[33] Additional renal activity and chronicity indices may help predict prognosis.[5]
Abdominal imaging
Ultrasound is indicated for severe abdominal pain to evaluate for intussusception or perforation. It may also be used to evaluate testicular pain and swelling.[29]
IgAV is associated with a wide range of GI features including gastritis, duodenitis, GI mucosal ulceration, and purpura. Periumbilical or epigastric pain is common, especially with meals, and although bleeding is generally occult, it can be associated with melena. Intussusception is the most common serious GI complication.[29][34]
Use of this content is subject to our disclaimer