Investigations
1st investigations to order
abdominal ultrasound
Test
Request ultrasound for any patient with suspected gallstone disease.[10]
Abdominal ultrasound has low sensitivity for choledocholithiasis, but its accuracy is better for any accompanying bile duct dilation.[91][90]
For acute calculous cholecystitis, abdominal ultrasound has high sensitivity for stones plus distension of the gallbladder lumen, gallbladder wall thickening, pericholecystic fluid, and a positive radiological Murphy sign.[90]
[Figure caption and citation for the preceding image starts]: Ultrasound of acute cholecystitis and presence of gallstones: the arrow points to a gallstone in the fundus of the gallbladder with its echogenic shadow belowCourtesy of Charles Bellows and W. Scott Helton; used with permission [Citation ends].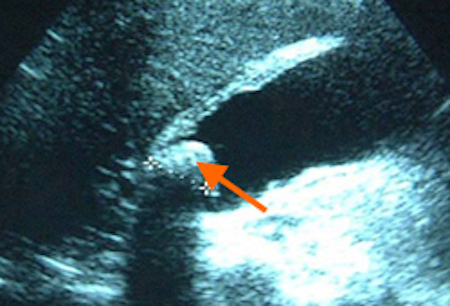 [Figure caption and citation for the preceding image starts]: Gallbladder ultrasound demonstrating cholelithiasis with characteristic shadowingCourtesy of Kuojen Tsao; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Gallbladder ultrasound demonstrating cholelithiasis with characteristic shadowingCourtesy of Kuojen Tsao; used with permission [Citation ends].
Result
cholelithiasis: stones in the gallbladder
choledocholithiasis: stones in the bile duct with or without bile duct dilation
serum LFTs
Test
Offer liver function tests to any patient with suspected gallstone disease.[10]
Result
uncomplicated cholelithiasis: normal
choledocholithiasis: elevated alkaline phosphatase; elevated bilirubin
brief biliary obstruction with subsequent stone passage: early, transient elevation in alanine aminotransferase before the alkaline phosphatase rises
FBC
Test
Take a full blood count to identify serious complications.
Result
normal WBC in simple (uncomplicated) biliary colic
elevated WBC in acute cholecystitis, cholangitis, or pancreatitis[1]
serum lipase or amylase
Test
Take blood to exclude pancreatitis if the patient’s pain is located primarily in the epigastric area, with or without radiation to the back. Serum lipase is the preferred test if available; lipase levels remain elevated for longer (up to 14 days after symptom onset vs. 5 days for amylase), providing a higher likelihood of picking up the diagnosis in patients with a delayed presentation.[84][85][86]
Result
elevated (>3 times upper limit of normal) in acute pancreatitis
Investigations to consider
magnetic resonance cholangiopancreatography (MRCP)
Test
Consider requesting MRCP if ultrasound has not detected common bile duct stones but you suspect choledocholithiasis because:[10]
The bile duct is dilated, and/or
Liver function test results are abnormal.
Note that MRCP has a sensitivity of 90% and specificity of 95% for the detection of bile duct stones; however, it has a reduced sensitivity (65%) to detect small (<5 mm) biliary stones.[93][94][97]
Result
stones in gallbladder or bile duct
endoscopic ultrasound scan (EUS)
Test
For ongoing clinical suspicion of choledocholithiasis (e.g., positive symptoms ± blood tests):[73]
If MRCP does not identify stones in the bile duct, or
After negative ultrasound if MRCP is contraindicated (e.g., in those with implanted devices or claustrophobia).
EUS is not suitable for patients who have had gastrointestinal bypass procedures.[27]
Result
stones in gallbladder or bile duct
abdominal CT scan
Test
If you suspect conditions other than gallstone disease, refer the patient for further investigations as necessary.[10]
Consider requesting an abdominal CT scan if the patient has biliary pain and an unremarkable abdominal ultrasound. This may identify potential complications of acute cholecystitis (e.g., emphysema of the gallbladder wall, abscess formation, perforation).[1] See Acute cholecystitis.
Result
may be normal or show stones in the gallbladder, and possibly in the bile or pancreatic ducts
acute cholangitis: bile duct dilation with choledocholithiasis
acute pancreatitis: diffuse or segmental enlargement of the pancreas
Use of this content is subject to our disclaimer