Investigations
1st investigations to order
upper gastrointestinal endoscopy
Test
Gastroscopy has low sensitivity for the diagnosis of early achalasia and may be reported as normal. However, it is an essential first-line investigation to exclude malignancy.[25]
In patients with a dilated oesophagus, a clear fluid diet for a prolonged period or oesophageal lavage may be required before endoscopy to avoid aspiration and to obtain adequate views. The gastro-oesophageal junction can be tight but gives way with sustained gentle pressure with the gastroscope.
Biopsies from the cardia should be performed to exclude pseudoachalasia.
Result
mucosa obscured by retained saliva with frothy appearance; in advanced cases oesophagus may be dilated and tortuous and contain food debris (sigmoid oesophagus)
barium swallow
Test
In early disease the swallow may be reported as normal. In advanced disease the dilated oesophagus may be tortuous and sigmoid-shaped with diverticula.
Fluoroscopy is often used during a barium swallow.[26]
Result
loss of peristalsis and delayed oesophageal emptying; dilated oesophagus that tapers smoothly to a beak-like narrowing at the gastro-oesophageal junction
high-resolution oesophageal manometry
Test
High-resolution manometry is more accurate than conventional manometry for the diagnosis of achalasia.[28][29] It has superseded conventional manometry and is now the gold standard for the diagnosis and sub-classification of achalasia into 3 discrete subtypes.[28][36]
A multi-sensory catheter is used that enables detailed pressure topography plotting of oesophageal motility.
In some patients with achalasia it might not be possible to pass the manometry catheter through the lower oesophageal sphincter.
Longitudinal muscle spasm and consequent oesophageal shortening can result in apparent pseudorelaxation with traditional manometry, but this problem does not arise with high-resolution manometry.[37]
Result
incomplete relaxation of the lower oesophageal sphincter with wet swallows and oesophageal aperistalsis are the two most important manometric criteria for the diagnosis of achalasia; high-resolution manometry defines three clinical subtypes of achalasia, which are classified using the Chicago criteria; type I: impaired lower oesophageal sphincter (LOS) relaxation without peristalsis, characterised by 100% failed contractions and no oesophageal pressurisations; type II: impaired LOS relaxation with pan-oesophageal pressurisation occurring in at least 20% of swallows; type III: impaired LOS relaxation with premature oesophageal contractions or distal peristalsis in at least 20% of swallows. The subtype of achalasia predicts the response to treatment
Investigations to consider
chest x-ray
Test
Appearance may suggest achalasia, but the test has a low sensitivity and is not diagnostic.
Result
absence of the gastric gas bubble and dilated oesophagus with an air-fluid level
radionucleotide oesophageal emptying studies
Test
This investigation can be used for monitoring response to therapy.[31]
Result
delayed oesophageal transit
timed barium oesophagogram
Test
Barium swallow in which multiple sequential films are shot at pre-set time intervals.
Simple technique that directly measures liquid oesophageal emptying.
Does not require any special equipment or expertise and is repeatable; therefore, can be used to assess the progress of the disease and the outcome of treatment.[32][33][Figure caption and citation for the preceding image starts]: Classic appearance of dilated oesophagus with tapered beak-like narrowing on barium studyFrom the collection of Dr Jin-Yong Kang; used with permission [Citation ends].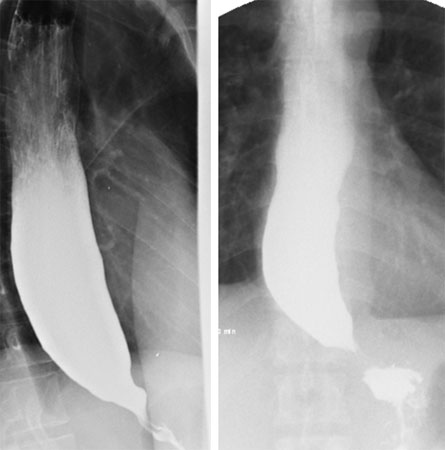
Result
delayed oesophageal transit
CT chest
Test
Used to rule out gastro-oesophageal infiltration by invading extrinsic or intrinsic malignancy.
Asymmetrical thickening may suggest pseudoachalasia.
Recommended in an older individual or if there is rapid or profound weight loss.
Result
dilation of the oesophagus; often concentric thickening of oesophageal wall
impedance planimetry
Test
To evaluate sphincter function by measuring changes in pressure with diameter and volume.[34][35] This can be utilised at the time of endoscopy or surgery at the gastro-oesophageal junction to measure the gastro-oesophageal junction distensibility using the functional luminal imaging probe (FLIP) device.
Result
may provide complementary information to high-resolution manometry where the diagnosis of achalasia is not clear and may provide peri-operative or endoscopic response to treatment in real-time.
Use of this content is subject to our disclaimer