Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
colonoscopy, device-assisted enteroscopy, and/or surgery
Colonoscopy or surgery may be appropriate in the absence of angiography. A colonoscopy is recommended to identify a lower gastrointestinal source of bleeding and to provide treatment. During this procedure, electrocautery, photocoagulation, clips, or an adrenaline (epinephrine) injection may be indicated to treat the lesion.
Careful treatment in the right colon is recommended, due to the thinner walls and higher risk for perforation.
Electrocautery uses heated probes to coagulate the bleeding lesions. Photocoagulation uses argon and Yag lasers and requires specific training.
[Figure caption and citation for the preceding image starts]: Endoscopic (device-assisted enteroscopy) image of small bowel angiodysplasia after treatment with argon plasma coagulationFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].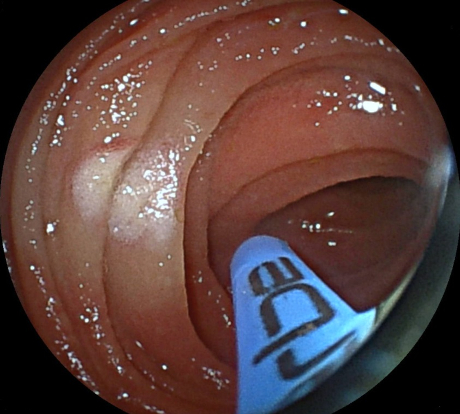 [Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends].
[Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends].
If the colonoscopy is negative and a small bowel source is suspected, device-assisted enteroscopy can be used to identify and treat the bleeding lesions. This can be done via the oral or retrograde route depending on the location of the suspected lesion in the small bowel.
Only patients with a large, life-threatening haemorrhage with little relief from interventional endoscopy or embolisation are appropriate for surgery.
At operation, if the patient is unstable, an on-table enteroscopy or blind sub-total colectomy may be appropriate.
Aortic valve replacement should be considered in patients with Heyde’s syndrome and ongoing bleeding.[8]
interventional endoscopy
During the endoscopy, electrocautery, photocoagulation, clips, or an adrenaline (epinephrine) injection may be indicated to treat the lesion.
Careful treatment in the right colon is recommended, due to the thinner walls and higher risk for perforation.
Electrocautery uses heated probes to coagulate the bleeding lesions. Photocoagulation uses argon and Yag lasers and requires specific training.[Figure caption and citation for the preceding image starts]: Endoscopic (device-assisted enteroscopy) image of small bowel angiodysplasia after treatment with argon plasma coagulationFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends].
wireless capsule enteroscopy or CT angiography + mesenteric angiography with embolisation or enteroscopy
If the endoscopy is negative and the bleeding continues, based on local expertise, capsule endoscopy or CT angiography should be performed which may guide further intervention. If CT angiography confirms active bleeding, it should be followed by a mesenteric angiography with a view to embolisation to treat the bleeding or endoscopic management using device-assisted enteroscopy if a small bowel source is seen.[40][51][Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].
repeat interventional endoscopy
If bleeding continues, a repeat endoscopy is recommended with therapeutic intervention. During the procedure, electrocautery, photocoagulation, clips, or an adrenaline (epinephrine) injection may be indicated to treat the lesion.
For patients with colonic angiodysplasias, careful treatment in the right colon is recommended, due to the thinner walls and higher risk for perforation.
For patients with recurrent small bowel bleeding, endoscopic management with device-assisted enteroscopy can be considered depending on the patient’s clinical course and response to prior therapy.[8]
Electrocautery uses heated probes to coagulate the bleeding lesions. Photocoagulation uses argon and Yag lasers and requires specific training.[Figure caption and citation for the preceding image starts]: Endoscopic (device-assisted enteroscopy) image of small bowel angiodysplasia after treatment with argon plasma coagulationFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer