Investigations
1st investigations to order
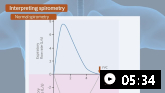
spirometry
Test
Performed in all children with suspected asthma who are able to give repeatable and reproducible results, which is dependent on their level of cooperation and age (typically from age 5 years).[111] The European Respiratory Society and American Thoracic Society (ERS/ATS) have jointly published standardised guidance for performing and interpreting spirometry.[112][113]
An obstructive pattern may be present, suggested by visual scalloping of the expiratory flow-volume loop. Decreases can be observed in the FEV₁/FVC ratio, FEV₁, or mid-flows (maximal expiratory flow at 25% of FVC [MEF25] or forced expiratory flow between 25% and 75% of FVC [FEF25-75]).
The FEV₁/FVC ratio is normally >0.90 in children.[1] FEV₁ and FEV₁/FVC results below the lower limit of normal (LLN) or below 80% of the predicted value are generally considered suggestive of an asthma diagnosis.[1][8][111] The LLNs for spirometry values are age-, height-, and ethnicity-dependent.[111][112][113]
The greater the variations in expiratory lung function, and the more often excess variation is observed, the more confident a clinician can be with the diagnosis of childhood asthma.[1] However, it is important to ensure that apparent variability does not reflect variations in technique over time, because both spirometry and PEF measures are effort-dependent.
False normal FEV₁/FVC ratios are possible with an incorrect technique, irrespective of age, and normal spirometry results do not automatically exclude asthma.[1][111]
See Diagnostic criteria for more detail.
A guide on how to perform and interpret spirometry, including common pitfalls.
Result
may show obstructive pattern
peak expiratory flow (PEF)
Test
An alternative to spirometry where spirometry is not available.
Measurement of the peak expiratory flow (PEF) is less reliable than spirometry, but its use is preferred where diagnosis would otherwise rely on symptoms only (see Diagnostic criteria).[1] A PEF lower than the age- and height-predicted normal range may be consistent with airway obstruction.
PEF criteria that show excess variability in expiratory lung function when diagnosing asthma in children include: positive bronchodilator responsiveness (≥15%); excessive diurnal variability in twice-daily measurements (>13%); improved lung function after 4 weeks of treatment (≥15%); and excessive variation in lung function between visits (≥15%).[1]
In a small proportion of children with poor symptom perception PEF may have a role in ongoing asthma management.
The greater the variations in expiratory lung function, and the more often excess variation is observed, the more confident a clinician can be with the diagnosis of childhood asthma.[1] However, it is important to ensure that apparent variability does not reflect variations in technique over time, because both spirometry and PEF measures are effort-dependent.
When used, record the highest of 3 PEF readings.

How to use a peak flow meter to obtain a peak expiratory flow measurement.
Result
may be low; may show excessive variability
response to bronchodilator
Test
Where spirometry is available, bronchodilator response should be assessed in all children with suspected asthma who are old enough to comply.
A >12% improvement in FEV₁ predicted is considered significant and suggestive of a diagnosis of asthma.[1][111] Of note, the ERS/ATS technical standard for routine lung function tests recommends a >10% improvement in the predicted FEV₁ or FVC for diagnosing bronchodilator reversibility consistent with asthma.[113]
Measurement of the peak expiratory flow (PEF) is an alternative to spirometry where spirometry is not available. Although the PEF is less reliable than spirometry, its use is preferred where diagnosis would otherwise rely on symptoms only.[1] A positive bronchodilator test result is an improvement of ≥15% on PEF testing.
Lack of response should be interpreted as evidence of an alternative diagnosis. More likely to obtain a true positive result if bronchodilator medication is withheld before testing (i.e., short-acting beta-agonist ≥4 hours, long-acting beta agonist 24-48 hours).
Result
shows reversibility
Investigations to consider
airway challenge tests
Test
Testing is considered in all children able to deliver reproducible spirometry when the diagnosis remains unclear following initial lung function testing.[111]
Tests are categorised as direct (methacholine, histamine) or indirect (mannitol, hypertonic saline) depending on how they act on airway smooth muscle.
The exact criteria of a positive test depend on the agent and guideline used: for methacholine, a fall in the FEV₁ of ≥20% from baseline indicates a positive result; for mannitol, a ≥15% fall from baseline indicates a positive result.[1][111]
Due to the presence of airway hyper-responsiveness in other chronic respiratory conditions (such as cystic fibrosis), the main value of airway challenge testing may be in its negative predictive value.
Result
FEV₁ decreased
exercise challenge test
Test
GINA considers a decrease in FEV₁ of >12% predicted, or a decrease in peak expiratory flow of >15% from baseline, to be significant and is consistent with a diagnosis of exercise-induced bronchoconstriction.[1]
European Respiratory Society paediatric guidelines state that a decrease in FEV₁ of >10% from baseline constitutes a positive test.[111]
Spirometry is measured at baseline and every 5 minutes after challenge for a total of 20 minutes. Exercise challenge testing should be considered in children from 5 years of age with exercise-related symptoms if asthma diagnosis cannot be confirmed with first-line tests.[111] The exercise challenge should be performed according to the recommended guidelines.
Result
FEV₁ or peak expiratory flow may be decreased
FBC
sweat test
Test
May be used to distinguish the presence of cystic fibrosis.
Sweat chloride 60 mmol/L or greater (60 mEq/L or greater) on repeat samples is diagnostic of cystic fibrosis. Values of 30 mmol/L (>30 mEq/L) are borderline.
Result
normal
sputum culture
Test
May be ordered when suspicion of bacterial lung infection exists.
Result
may grow bacteria with infection
skin prick testing
Test
May be used to support the presence of an atopic state.
Should not be used to diagnose asthma.[111]
Result
may be abnormal
chest x-ray
Test
May show hyperinflation. Helps distinguish from other cardiac and pulmonary diseases such as cardiac failure, bronchiectasis (when severe), or situs inversus.
Result
normal or may show hyperinflation
electron micrograph ciliary studies
Test
May be ordered when primary ciliary dyskinesia is suspected, including Kartagener's syndrome (situs inversus with unusually positioned gastric bubble)
Result
normal
chest CT
Test
May show hyperinflation or other causes of pulmonary abnormality or small airways disease that can present with wheeze (e.g., bronchiolitis obliterans). Can distinguish cardiac from pulmonary diseases.
Not recommended routinely, to predict treatment outcomes or lung function, or to assess treatment response.
Result
normal or may show hyperinflation, bronchiectasis, bronchiolitis obliterans, or situs inversus
sinus CT
Test
Can show evidence of chronic rhinosinusitis and nasal polyps, which are associated with more severe asthma. The presence of chronic rhinosinusitis with nasal polyposis can also help identify candidates for biological therapy.
Not recommended routinely.
Result
normal or may show opacification of involved sinuses, mucosal thickening, air-fluid levels, or anatomic abnormalities such as polyps
bronchoscopy
Test
May be done in the case of foreign body aspiration, or when structural abnormalities are suspected (e.g., tracheomalacia or bronchomalacia) that can also present with wheeze.
Result
typically normal
Emerging tests
fractional expired nitric oxide (FeNO)
Test
Some guidelines state that an elevated fractional exhaled nitric oxide (FeNO) may be used to support a diagnosis of asthma.[100][122] Others consider that there is a lack of evidence to support the routine use of FeNO.[8] Clinician-led guidelines agree that FeNO levels are not diagnostic on their own, and GINA states that further studies are still needed to guide recommendations on FeNO use.[1][8][111][122][123][124]
Although FeNO is modestly associated with some markers (sputum and blood eosinophil levels), levels vary depending on a range of patient factors (including age and height), meaning that it cannot be used in isolation to diagnose or exclude asthma. For example, levels are known to be higher in type 2 airway inflammation and some non-asthma conditions (e.g., eosinophilic bronchitis, atopy, allergic rhinitis, eczema); normal in other asthma phenotypes (e.g., neutrophilic asthma); lower in smokers, during bronchoconstriction, and the early phases of an allergic response; and can be either increased or decreased during viral respiratory infections.[1] FeNO levels are also influenced by ethnicity, and to this end, a look-up table has been proposed.[125]
Result
elevated
Use of this content is subject to our disclaimer