Investigations
1st investigations to order
conventional radiographs
Test
Conventional radiographs should be ordered in patients with suspected osteosarcoma. The radiographs should ideally be reviewed by a consultant musculoskeletal radiologist. [Figure caption and citation for the preceding image starts]: Conventional radiograph, anteroposterior view; poorly circumscribed, permeative lesion involving distal femoral metaphysis with mixed radiodense and radiolucent appearance; a large soft tissue mass with periosteal reaction is also presentPersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].
Result
radiolucent lesion with areas of mottled radiodensity and ill-defined margins; neoplasm is usually located in the metaphysis of long bone; periosteal reaction in the form of Codman's triangle or a sunburst appearance is common; sometimes soft tissue mass can be appreciated on conventional radiographs
bone biopsy
Test
Histological examination of biopsy sample confirms a diagnosis of osteosarcoma.[23][Figure caption and citation for the preceding image starts]: Osteoblastic osteosarcoma; lace-like osteoid in a highly pleomorphic sarcomatous stromaPersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].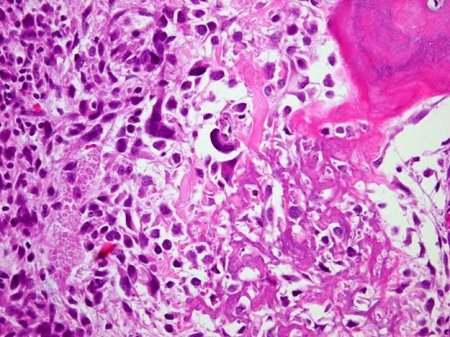
Biopsies should be taken as part of the initial workup for patients aged under 40 years, or after local staging in patients aged over 40 years.[23] Guidelines recommend consultation with an orthopedic oncologist on appropriate pre-biopsy imaging.[23]
Core needle or open biopsy at a specialised centre in the management of osteosarcoma are recommended techniques for biopsy.[23] Fine-needle aspiration and excisional biopsies are not recommended. Tissue should be submitted for pathological assessment as quickly as possible. Tumour imprints (touch preps) can be taken, and tissue should be snap-frozen and/or sent for cytogenetic analysis.
Result
highly pleomorphic spindle cell neoplasm producing osteoid or immature bone; osteoid typically has a lace-like appearance; neoplastic cells and osteoid show a permeative growth pattern with invasion of the native bone trabeculae; neoplastic cartilage can also be produced by the tumour cells; mitotic activity is high and composed of atypical mitotic figures
magnetic resonance imaging (MRI)
Test
An MRI with gadolinium contrast is the test of choice to evaluate tumour extension within the bone and soft tissue. It also identifies skip metastases.[23][Figure caption and citation for the preceding image starts]: Magnetic resonance imaging, coronal view; osteosarcoma of distal femur showing low-intensity signal; T1-weighted image; actual intra-osseous and extra-osseous tumour extent is also appreciatedPersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].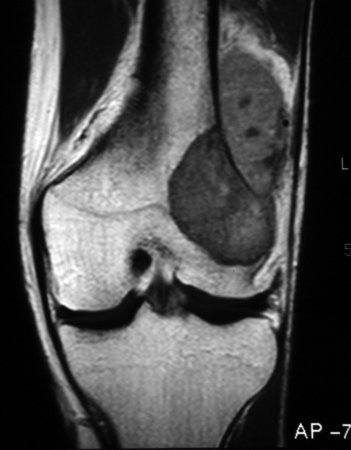 [Figure caption and citation for the preceding image starts]: Magnetic resonance imaging, axial view; osteosarcoma of distal femur showing high-intensity signal; T2-weighted imagePersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].
[Figure caption and citation for the preceding image starts]: Magnetic resonance imaging, axial view; osteosarcoma of distal femur showing high-intensity signal; T2-weighted imagePersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].
MRI (with and without contrast) or CT (with contrast) are recommended of the skeletal metastatic sites.[23]
Result
low signal on T1-weighted images; high signal on T2-weighted images; fluid levels
computed tomography (CT)
Test
Matrix production by the tumour and the extent of cortical destruction are best appreciated on CT scans. A CT-guided biopsy can be performed simultaneously. If the tissue obtained is diagnostic, an open biopsy is not necessary and a treatment plan can be designed. If the tissue obtained is not diagnostic, an open biopsy is required.[Figure caption and citation for the preceding image starts]: Computed tomographic scan, axial view; osteosarcoma of proximal tibia; matrix production and bone destruction are best appreciated on conventional tomographsPersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].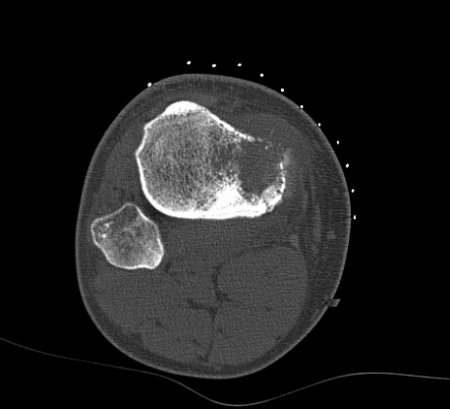
MRI (with and without contrast) or CT (with contrast) are recommended of the skeletal metastatic sites.[23]
Result
findings vary with exact type of tumour; shows dense bony mass; may show central calcification, cortical destruction
CT thorax
bone scan
Test
Usually uses technetium-99. Forms part of the secondary staging. Will reveal approximate extent of primary lesion and highlight any skip or distant metastases.[Figure caption and citation for the preceding image starts]: Bone scan; high radionuclide uptake at tumour sitePersonal collections of Dr Michael J. Klein and Dr Luminita Rezeanu [Citation ends].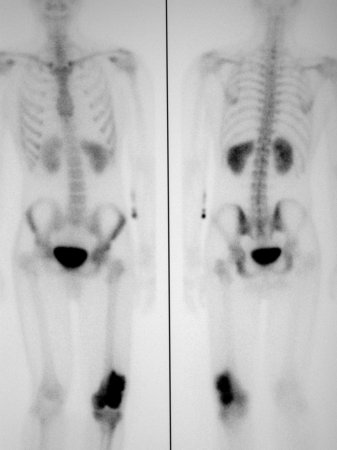 Suspected metastatic disease should be further evaluated with CT or MRI.[23]
Suspected metastatic disease should be further evaluated with CT or MRI.[23]
Result
intensely hot signal at primary tumour site; may also identify skip or distant metastases
whole body fluorodeoxyglucose (FDG)-PET/CT
full blood count
Test
A full blood count with differential is recommended as part of the workup for osteosarcoma.[23]
Result
normal
serum alkaline phosphatase
Test
Although it is common, an elevated serum level is not diagnostic of osteosarcoma. Serum values tend to normalise after tumour ablation and resurge with local recurrence or metastatic disease.
Result
usually elevated
serum lactate dehydrogenase
Test
Levels are frequently elevated but are not diagnostic of osteosarcoma. However, elevated levels in combination with typical signs and symptoms increases the suspicion of a bone lesion.
Result
usually elevated
Use of this content is subject to our disclaimer