Case history
Case history
A 78-year-old man with a history of hypertension presents to his primary care physician with 1 episode of dizziness while watching television. On physical examination, his heart rate is measured at about 40 bpm. A 12-lead ECG is obtained showing sinus rhythm at about 75 bpm and complete heart block with a wide escape rhythm at about 40 bpm.[Figure caption and citation for the preceding image starts]: Third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].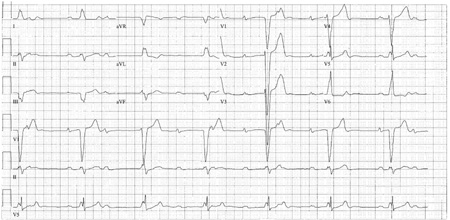 [Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Third-degree heart block: right bundle-branch block escapeCourtesy of Dr Sanjiv Petkar; used with permission [Citation ends].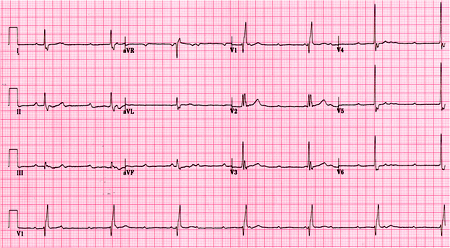 On further questioning, the patient admits to increasing fatigue and dyspnoea on exertion for the past few weeks. Notably, the patient has bifascicular block at baseline (right bundle-branch block and left anterior fascicular block).[Figure caption and citation for the preceding image starts]: Baseline ECG for a patient with third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].
On further questioning, the patient admits to increasing fatigue and dyspnoea on exertion for the past few weeks. Notably, the patient has bifascicular block at baseline (right bundle-branch block and left anterior fascicular block).[Figure caption and citation for the preceding image starts]: Baseline ECG for a patient with third-degree AV blockCourtesy of Dr Susan F. Kim, Dr John F. Beshai, and Dr Stephen L. Archer; used with permission [Citation ends].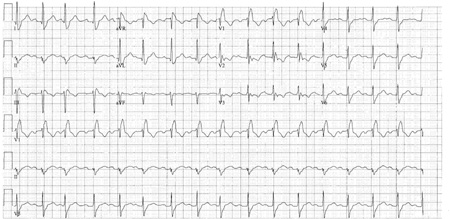
Other presentations
The degree of AV block and the severity of symptoms are not necessarily directly related. For example, patients with complete (third-degree) AV block may be minimally symptomatic or completely asymptomatic. Ultimately, these patients may be diagnosed incidentally on undergoing an evaluation for other reasons. On the other hand, patients with type I second-degree AV block may be very symptomatic, presenting with syncope or pre-syncope due to very slow ventricular rates. AV block may also occur in the setting of other acute illnesses such as an acute coronary syndrome, severe electrolyte or pH disturbances, or severe hypoxaemia. AV block of any degree may also occur in post-cardiac surgery patients and in patients with Lyme disease.
Use of this content is subject to our disclaimer