Investigations
1st investigations to order
serum 25-hydroxyvitamin D
Test
25-hydroxyvitamin D is the major circulating form of vitamin D used to determine vitamin D status.[2]
Some assays measure both 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3; the total of both of these is what is important.
The 25-hydroxyvitamin D test should not be used as a screening test. However, if a child or adult has one or more of the risk factors or signs and symptoms of vitamin D deficiency, this blood test should be obtained to confirm the diagnosis and to rule out other potential causes for vitamin D deficiency, such as syndromes due to acquired or inherited disorders of vitamin D metabolism or phosphorus metabolism.
Result
vitamin D deficiency: ≤50 nanomoles/L (≤20 nanograms/mL); vitamin D insufficiency: between 52-72 nanomoles/L (21-29 nanograms/mL)
serum calcium
Test
Usually normal (unless long-standing vitamin D and calcium deficiency) due to secondary hyperparathyroidism, which mobilises calcium from the skeleton and conserves calcium in the kidney to maintain serum calcium within normal range.
May be decreased with inherited disorders of vitamin D metabolism such as pseudovitamin D-deficiency rickets and vitamin D-resistant rickets.
Result
normal
fasting serum phosphate
Test
Due to secondary hyperparathyroidism causing phosphaturia. However, if the serum phosphate level is not obtained in the fasting state, it provides little information about the actual phosphate status of the patient.
Result
low-normal or rarely low
serum alkaline phosphatase
Test
Usually high in rickets and osteomalacia. Elevated levels may indicate a high bone turnover state.
Result
normal or elevated
plain-film radiographs of knees and wrists
Test
Should be performed when rickets or osteomalacia is suspected.[78] Widening of the epiphyseal plate, and loss of definition of the zone of provisional calcification at the epiphyseal/metaphyseal interface, are early signs of rickets. [Figure caption and citation for the preceding image starts]: X-rays of a wrist from a child with vitamin D-deficiency rickets before (left panel) and after (right panel) treatment with vitamin DFrom the collection of M.F. Holick, PhD, MD; used with permission [Citation ends].
Looser's pseudofractures, which lie perpendicular to the cortical margins with the characteristic sclerotic borders, are a pathognomonic finding in osteomalacia.[79][Figure caption and citation for the preceding image starts]: Radiograph of the femoral shaft in a patient with osteomalacia demonstrating a 'pseudofracture' (also known as Looser's zone) on the medial aspect of the mid-femoral shaftFrom the collection of Bridget Sinnott, MD [Citation ends].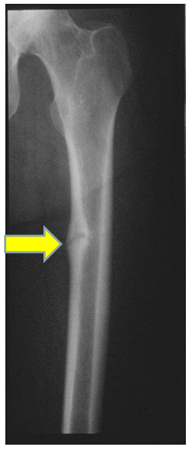
Result
cupping, splaying, and fraying of the metaphysis; Looser's zone (pseudofracture)
Investigations to consider
intact PTH
Test
Usually elevated in chronic severe vitamin D deficiency (osteomalacia and rickets). However, in mild vitamin D deficiency and insufficiency, intact PTH levels are usually normal. Therefore, PTH is not a good surrogate for vitamin D deficiency (diagnostic marker). Furthermore, if the patient is also magnesium-deficient they are unable to mount a PTH response to vitamin D deficiency and, therefore, have a normal intact PTH level.
Consequently this test should only be obtained when calcium is elevated, to help rule out causes of vitamin D deficiency such as primary hyperparathyroidism.
Result
normal or elevated
serum 1,25-dihydroxyvitamin D
Test
Should not be used to determine vitamin D status. However, this measurement is of great value in distinguishing the inherited and acquired disorders of vitamin D metabolism.
Patients with pseudovitamin D-deficiency rickets and vitamin D-resistant rickets often have a normal serum level of 25-hydroxyvitamin D. However, 1,25-dihydroxyvitamin D level differs, and is either low or undetectable in pseudovitamin D-deficiency rickets and very elevated in patients with vitamin D-resistant rickets.
Patients with X-linked hypophosphataemic rickets, autosomal-dominant hypophosphataemic rickets, and oncogenic osteomalacia have low levels of serum 1,25-dihydroxyvitamin D and phosphorus. This combination is pathognomonic for these conditions.
Result
normal or elevated
bone density (DEXA) scan
Test
Adults with chronic vitamin D deficiency may have a low bone density due to increased serum PTH, which removes matrix and mineral, causing osteopenia and ultimately osteoporosis. In addition, the mineralisation defect of the skeleton caused by vitamin D deficiency can result in a lower bone density.
Result
low bone density
Use of this content is subject to our disclaimer