Investigations
1st investigations to order
semen analysis
Test
Male aetiologies are detected in 27.8% of assisted reproductive technology (ART) cycles.[10] Male evaluation with at least a semen analysis is necessary while evaluating the female partner.
Result
may be normal; may reveal common single abnormalities or a combination of abnormalities such as asthenozoospermia (the percentage of progressively motile sperm below the reference limit of 32%), oligozoospermia (the total number or concentration of sperm below reference limit of 15 million sperm/mL), or azoospermia (no sperm in ejaculate)
luteal-phase progesterone
Test
A retrospective test of ovulation. Women with regular cycles do not routinely require additional tests to confirm ovulation, but they may be considered in women with hirsutism or when menstrual history is indeterminate.[2][80]
Serum is assessed 7 days after the presumed day of ovulation (or 7 days before the presumed menstrual cycle). A progesterone value >9.5 nmol/L (>3 ng/mL) is indicative of an ovulatory cycle. The timing of this test is critical.[80] The use of peak values has low sensitivity and specificity. However, any rise of progesterone concentration in the luteal phase is suggestive of ovulation, and thus further sampling (earlier in a short cycle, through to menses in a longer cycle) is considered confirmatory if the first value is indeterminate.
Result
<9.5 nmol/L (<3 ng/mL) if anovulatory
urinary luteinising hormone (LH)
Test
Ovulation can be detected prospectively with urinary LH prediction kits. Women with regular cycles do not routinely require additional tests to confirm ovulation, but they may be considered in women with hirsutism or when menstrual history is indeterminate.[2][80] LH prediction kits also provide a prospective assay of ovulation that can be used to time intercourse.
LH rises abruptly for approximately 18 hours before it peaks, and ovulation typically occurs about 36 hours after the onset of the surge. These tests are more accurate at predicting/demonstrating ovulation than basal body temperature charting (no longer recommended in the UK by the National Institute for Health and Care Excellence) and other measures.[82]
Result
a positive test kit result indicates imminent ovulation
transvaginal ultrasound scan
Test
As an extension to physical examination, a transvaginal ultrasound scan (TVUS/S) is often undertaken in the clinic setting.
A TVUS/S enables the assessment of pelvic organs, including the ovaries. It also enables the assessment of ovarian mobility and/or accessibility for oocyte retrieval if indicated ultimately.
A TVUS/S informs the decision for further detailed pelvic assessment.
Result
may demonstrate follicular development, polycystic appearance of ovaries, presence of significant cysts (including endometriomas), abnormal uterine structure (e.g., with congenital abnormalities), presence of fibroids, endometrial polyps, hydrosalpinges, adenomyosis
chlamydia antibody testing
Test
May be considered as an initial, non-invasive test to assess the risk for tubal occlusion.[2] A negative result suggests a low risk for tubal occlusion, but it does not rule out occlusion due to other infections. A positive result should be followed by further evaluation of tubal patency.[2][80]
Result
may be positive
hysterosalpingogram
Test
The assessment of tubal patency with hysterosalpingography is commonly undertaken in an outpatient setting. Women undergoing this test should be instructed to take a non-steroidal anti-inflammatory before the examination to reduce cramping. According to one individual patient data meta-analysis, hysterosalpingography (HSG) has a pooled sensitivity of 53% and a pooled specificity of 87% for identification of any tubal pathology.[88]
[Figure caption and citation for the preceding image starts]: Normal hysterosalpingography (HSG)From the collection of Dr Jared C. Robins [Citation ends]. [Figure caption and citation for the preceding image starts]: Hysterosalpingography (HSG) demonstrating bilateral hydrosalpingesFrom the collection of Dr Jared C. Robins [Citation ends].
[Figure caption and citation for the preceding image starts]: Hysterosalpingography (HSG) demonstrating bilateral hydrosalpingesFrom the collection of Dr Jared C. Robins [Citation ends].
Because the positive predictive value of HSG is low, results suggesting tubal obstruction might require further evaluation.[80]
Use of an oil-soluble contrast media for tubal flushing in the assessment of tubal patency may increase clinical pregnancy rates, and it is recommended over water-soluble contrast media.[2][91][92] The most common complication of oil-soluble contrast HSG is intravasation.[93] Oil embolism is a rare complication, but the technique should be performed with fluorescence guidance.[2]
Result
fallopian tubes: patent or blocked, with free spill of dye and normal tubal pattern; uterus: normal or abnormal contour, presence or absence of filling defects
hysterosalpingo-contrast sonography (HyCosY)
Test
A useful test without radiation exposure.
Opaque medium is instilled transcervically during transvaginal ultrasound scan to delineate the endometrial cavity and fallopian tubes.[89] HyCosY has a pooled sensitivity of 93% (95% CI 90% to 95%) and a pooled specificity of 90% (95% CI 87% to 92%) for the assessment of tubal patency.[90]
Result
tubes: patent or blocked, with free spill of contrast and normal tubal pattern; uterus: normal or abnormal contour, presence or absence of filling defects
basal follicle-stimulating hormone (FSH)
Test
A test of ovarian reserve that is performed on day 2-5 of the menstrual cycle. The test is predictive of how well patients may respond to treatment. However, except when the FSH is very high, the test is not predictive of achieving pregnancy or failure to conceive, especially in young women. This means this test should only be used to determine whether a patient will require higher doses of medications to achieve ovarian stimulation (e.g., in a patient with a relatively elevated FSH, gonadotrophin therapy may be favoured over clomifene). Because of the variability of reproductive cycles, basal FSH levels can vary and so unless the FSH value is very high, abnormal tests should be repeated.
FSH can be assessed randomly in amenorrhoeic women.
Gonadotrophin values can significantly vary among laboratories.
Result
<2 international units (IU)/L is compatible with hypogonadotrophinism; <4 IU/L may be considered predictive of a high response to future ovarian stimulation; >8.9 IU/L may be considered predictive of a low response to future ovarian stimulation; >10 IU/L indicates possible reduced ovarian reserve; >30 IU/L indicates a menopausal level or pre-ovulatory surge (interpret findings with consideration of the clinical picture)
saline infusion sonogram
Test
Saline-infusion sonography (SIS) can be used to follow up intrauterine abnormalities seen on hysterosalpingography (HSG) or evaluate the uterus if there is no suspicion about the fallopian tubes. Intrauterine lesions suggested by HSG can be further evaluated with saline infusion sonogram (SIS or hysterosonogram). The sensitivity and specificity of SIS were both estimated to be nearly 100% when surgery was used as a definitive test.[94][95][Figure caption and citation for the preceding image starts]: Normal saline infusion ultrasoundFrom the collection of Dr Jared C. Robins [Citation ends]. [Figure caption and citation for the preceding image starts]: Saline infusion ultrasound with polypFrom the collection of Dr Jared C. Robins [Citation ends].
[Figure caption and citation for the preceding image starts]: Saline infusion ultrasound with polypFrom the collection of Dr Jared C. Robins [Citation ends].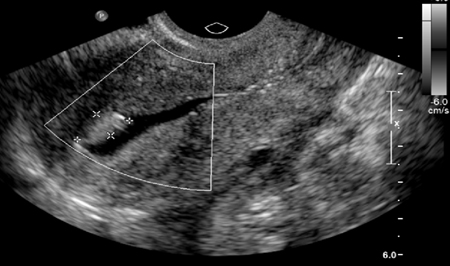
Result
may show intrauterine lesion
antral follicle count
Test
A total antral follicle count undertaken by transvaginal ultrasound assessment is performed on day 3 of the menstrual cycle.
Result
<5-7 oocytes may be considered consistent with diminished ovarian reserve; ≤4 oocytes may be considered predictive of a low response to future ovarian stimulation
serum anti-Müllerian hormone (AMH)
Test
AMH can be measured on any day of the menstrual cycle.[101] AMH levels correlate well with basal FSH levels and response to stimulation, meaning it may prove to be a better predictor of treatment response and pregnancy. It may also improve ovarian reserve testing when used in combination with other tests.
Result
<7.1 pmol/L (<1 ng/mL) may be considered consistent with diminished ovarian reserve; ≤5.4 pmol/L (≤0.76 ng/mL) may be considered predictive of a low response to future ovarian stimulation
Investigations to consider
serum LH
Test
If ovulation is not confirmed using initial tests, further diagnostic tests are indicated to establish the cause, including assessment of FSH and LH (to detect hyper-gonadotrophic or hypogonadotrophic hypogonadism).
Serum LH is performed randomly with FSH in amenorrhoea.
Result
<2 IU/L is compatible with hypogonadotrophinism; >30 IU/L indicates a menopausal level
serum oestradiol
Test
Basal FSH and oestradiol can be measured together in the early follicular phase to assess ovarian reserve; however, serum oestradiol (E2) should not be measured in isolation to predict the outcome of fertility treatment.[1][80] Elevated oestradiol levels may suppress FSH levels, so the value of measuring oestradiol levels is that they provide context for normal FSH levels. High oestradiol levels are, therefore, associated with reproductive ageing and diminished ovarian reserve. Performed randomly in an amenorrhoeic woman.
Result
<184 pmol/L (<50 pg/mL) is basal, suggesting little or no ovarian activity at the time of testing; >220-294 pmol/L (>60-80 pg/mL) in the early follicular phase can indicate reproductive ageing and hastened oocyte development
free serum testosterone
Test
If ovulation is not confirmed using initial tests, further diagnostic tests are indicated to establish the cause, including assessment of free testosterone (to detect polycystic ovary syndrome or other causes of hyper-androgenism).
Result
may be elevated with polycystic ovary syndrome or other causes of hyper-androgenism
serum TSH
Test
To assess for thyroid dysfunction as a possible cause of infertility.
Result
may be abnormal if there is associated thyroid disease
coeliac disease testing
Test
To assess for coeliac disease as a possible cause of infertility.
First-line screening usually consists of immunoglobulin A-tissue transglutaminase (IgA-tTG) and quantitative IgA serology. Before testing, it is crucial to ensure that the patient is ingesting gluten, because all diagnostic tests will usually normalise on a gluten-free diet.
Result
may be positive if there is associated coeliac disease
serum prolactin
Test
If ovulation is not confirmed using initial tests, then further diagnostic tests are indicated to establish the cause, including assessment of prolactin (to help detect pituitary tumour).
May also be elevated with idiopathic hyper-prolactinaemia or in the setting of use of dopamine antagonists such as antipsychotic agents.
Result
may be elevated if micro- or macroprolactinoma, or other pituitary tumour present
3-dimensional ultrasonography
Test
Three-dimensional (3D) ultrasound has emerged as the imaging tool of choice for the assessment of the female pelvis. A 3D ultrasound scan enables a more detailed evaluation of the uterus, with reconstruction of anatomical planes, elusive to conventional TVUS/S.[86]
Result
may show intrauterine lesions
pelvic MRI
Test
Historically, MRI was the preferred method of assessment for uterine abnormalities, predominantly Müllerian duct anomalies. MRI has been reported to have 100% specificity and 80% to 100% sensitivity for the evaluation of pelvic anomalies.[84][85]
The production of images in multiple planes makes MRI an excellent pre-operative assessment before reproductive gynaecological surgeries such as myomectomy or metroplasty.
Result
may show uterine/adnexal abnormality; if used by a radiologist with special interest in gynaecology, an additional benefit of MRI includes non-surgical assessment of the presence and severity of endometriosis, such as deep infiltrating disease
laparoscopy and hysteroscopy
Test
Women at risk of tubal obstruction can be offered laparoscopy or hysteroscopy to provide information about peri-tubal adhesions or endometriosis.[1][80] The decision to perform laparoscopy as an initial diagnostic modality is based on clinical suspicion. For example, in a woman with a history of cyclic pelvic pain suggestive of endometriosis, laparoscopy may be the best initial evaluation.
In selected cases, hysteroscopy at the time of laparoscopy may be indicated (e.g., to clarify uterine abnormalities or assess submucous fibroids). In addition to direct visualisation for diagnostic purposes, laparoscopy and hysteroscopy may also confer the benefit of surgical treatment at the same time. Some evidence suggests that hysteroscopy may improve live birth rates in women undergoing assisted reproductive technology, even when initial imaging is normal.[97][98] However, one Cochrane review noted that results were inconclusive when only considering trials at low risk of bias, and guidelines recommend against hysteroscopy when imaging is normal.[2][99]
[ ![]() ]
[Evidence C]
]
[Evidence C]
Result
may show abnormal anatomical findings
karyotyping
Test
May be considered as an additional test in women with amenorrhoea.
Result
may demonstrate chromosomal abnormality (e.g., with Turner’s syndrome or Robertsonian translocation)
Use of this content is subject to our disclaimer