Investigations
1st investigations to order
skin biopsy for histopathological evaluation with light microscopy
Test
A newly formed blister should be biopsied, if possible, in its entirety. If the blisters are too large, the edge of an existing blister should be biopsied, taking care not to traumatise the tissue so that the epidermis does not separate from the dermis during the sampling process. In the prodromal, non-bullous phase or in atypical cases, the light microscopy findings may be less specific, rendering only eosinophilic spongiosis and focal (if any) sub-epidermal clefts. If the patient has newly formed blisters and the first attempt does not yield a characteristic finding, the test may be repeated.[Figure caption and citation for the preceding image starts]: Light microscopy: sub-epidermal blisterFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].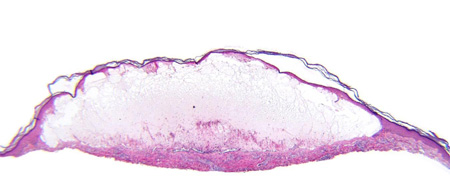 [Figure caption and citation for the preceding image starts]: Fibrin network is present in the blister cavity while the dermal infiltrate contains many eosinophilsFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].
[Figure caption and citation for the preceding image starts]: Fibrin network is present in the blister cavity while the dermal infiltrate contains many eosinophilsFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].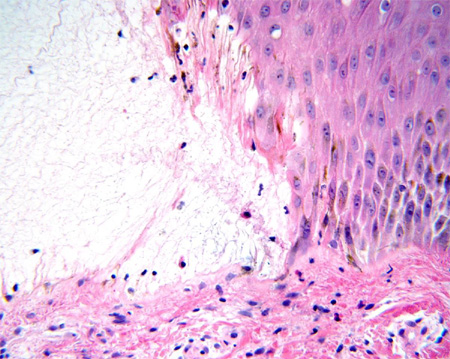 [Figure caption and citation for the preceding image starts]: Fibrin and eosinophils are present in the blister cavityFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].
[Figure caption and citation for the preceding image starts]: Fibrin and eosinophils are present in the blister cavityFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].
Result
sub-epidermal blister with dermal inflammatory cell infiltrate rich in eosinophils
skin biopsy for direct immunofluorescence testing
Test
Skin biopsy for direct immunofluorescence testing is the best available test. Normal, uninvolved skin adjacent to a blister (peri-lesional) should be biopsied. The specimen needs to be either snap-frozen or placed in Michel's medium and transported to an appropriate laboratory that performs immunopathological testing. Improper handling of the specimen may lead to a false-negative result. If, however, a true-negative result is received, additional tests are warranted to further clarify the diagnosis. A positive result should be confirmed by indirect immunofluorescence testing.[Figure caption and citation for the preceding image starts]: Linear band of IgG at the basement membrane zoneFrom the collection of Dr Vesna Petronic-Rosic [Citation ends].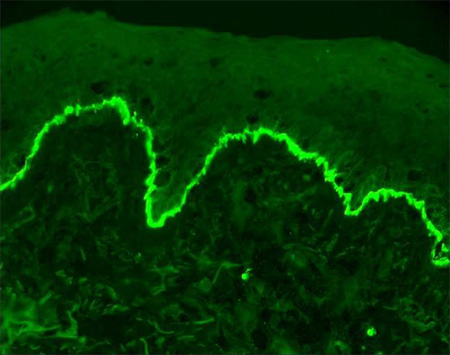
Result
linear band of IgG and/or C3 (and rarely other Ig classes) along the basement membrane zone
indirect immunofluorescence test on serum
Test
Indirect immunofluorescence testing for antibodies to bullous pemphigoid antigens is performed in specialised laboratories on serum. This test is performed if the direct immunofluorescence result is positive.
The test is positive in up to 96% of patients.[34] Previous immunosuppressive therapy may result in a lower or negative titre, which does not correlate with the clinical activity of the disease.
Result
positive titre for antibodies to bullous pemphigoid antigens
Investigations to consider
ELISA test
Test
ELISA has been found to be highly specific and sensitive for the detection of specific bullous pemphigoid antigens.[31] It should be ordered if the direct and indirect immunofluorescence studies do not yield characteristic diagnostic information. ELISA kits for testing bullous pemphigoid antigen-specific IgG auto-antibodies are available commercially, but only a few medical centres offer this service.
Result
determination of a specific region of the bullous pemphigoid antigens (e.g., the NC16A domain of BP180)
Emerging tests
immunoblotting
Test
The sensitivity of immunoblotting varies. In 75% of patients, a reaction occurs with the BP230 antigen, while in 50% of patients, a reaction occurs with the BP180 antigen.[32] Immunoblotting or Western blotting demonstrates reactivity of IgG in the sera of patients with proteins extracted from healthy human skin.[9]
Result
reactivity of IgG in the sera
immunoprecipitation
Test
Immunoprecipitation detects auto-antibodies specific for BP230 and BP180.[9] Unlike immunoblotting, immunoprecipitation is performed with native, rather than denatured, protein and is more sensitive.
Result
reactivity with BP230 and BP180
fluorescence overlay antigen mapping (FOAM) technique
Test
The FOAM technique is not routinely available. It facilitates differential diagnosis of the acquired sub-epidermal bullous skin disorders, bullous pemphigoid, and epidermolysis bullosa acquisita, in which ultrastructural identification of the skin site with skin-bound IgG deposits at the epidermal basement membrane zone may be essential to the correct diagnosis.[33]
Result
digitalised multicolour FOAM images of peri-lesional skin from patients with bullous pemphigoid show non-overlap band patterns of green-stained lamina lucida IgG deposits and red-stained type VII collagen
Use of this content is subject to our disclaimer