Case history
Case history #1
A 55-year-old man presents with tingling of the left hand and loss of sensation in both lower limbs. He gives a 6-week history of a 5-kg weight loss and fevers. Examination shows mononeuritis multiplex affecting both the common peroneal nerves and the left radial nerve. Investigation reveals a normocytic, normochromic anaemia (haemoglobin 93 d/L [9.3 g/dL]), neutrophilia (WBC count 11.5 x 10⁹/L [11,500/microL]), a raised creatinine (2.48 mg/dL), and elevated inflammatory markers (erythrocyte sedimentation rate [ESR] 89 mm/hour, CRP >15.2 nanomol/L [1.6 mg/L]) but normal urinary sediment. Tests are negative for anti-neutrophil cytoplasmic antibodies (ANCA), with no evidence of hepatitis B infection. His blood pressure is 193/103 mmHg. Sural nerve biopsy demonstrates a transmural vascular inflammatory infiltrate with a mixture of macrophages, lymphocytes, and neutrophils plus evidence of focal and segmental necrotising vasculitis with fibrinoid necrosis. Multiple aneurysms are seen on renal angiography.[Figure caption and citation for the preceding image starts]: Renal angiogram showing aneurysms, a classical feature of PANFrom the collection of Dr Raashid Luqmani [Citation ends]. [Figure caption and citation for the preceding image starts]: Renal angiogram showing aneurysms and microaneurysmsFrom the collection of Dr Loic Guillevin [Citation ends].
[Figure caption and citation for the preceding image starts]: Renal angiogram showing aneurysms and microaneurysmsFrom the collection of Dr Loic Guillevin [Citation ends].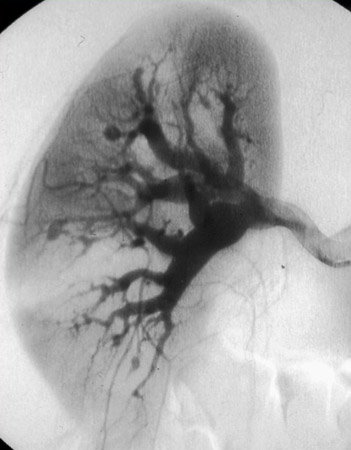
Case history #2
A 44-year-old woman presents with a 3-month history of abdominal pain, fever, and weight loss. The abdominal pain is cramping in nature and occurs 30 minutes after eating. Abdominal examination is unremarkable. She has widespread purpuric lesions on her lower limbs. Blood tests reveal elevated inflammatory markers (ESR 93 mm/hour, CRP >15.2 nanomol/L [1.6 mg/L]) and raised transaminases (ALT 300 units/L). ANCA is negative. HbeAg and HbsAg are positive, with raised hepatitis B DNA. A liver ultrasound examination is normal. A full-thickness skin biopsy of the purpuric lesions is reported as showing segmental necrotising vasculitis of medium vessels with fibrinoid necrosis. A mesenteric angiogram demonstrates multiple aneurysms involving the superior and inferior mesenteric arteries. [Figure caption and citation for the preceding image starts]: A purpuric rash is a common featureFrom the collection of Dr Loic Guillevin [Citation ends].
Other presentations
Testicular pain due to ischaemic orchitis is a classical feature of polyarteritis nodosa (PAN) but is rare at presentation. Some patients may present with an acute surgical abdomen resulting from infarction of bowel, liver, spleen, or pancreas. Myocardial infarction, ischaemic cardiomyopathy, optic ischaemia, and ischaemic complications of the female genital tract are possible but unusual.
Use of this content is subject to our disclaimer