History and exam
Key diagnostic factors
common
presence of risk factors
Make an assessment of risk factors for IE. These include:[30]
Acquired valvular heart disease with stenosis or regurgitation
Hypertrophic cardiomyopathy
Previous infective endocarditis
Structural congenital heart disease, including surgically corrected or palliated structural conditions, but excluding isolated atrial septal defect, fully repaired ventricular septal defect, fully repaired patent ductus arteriosus, and closure devices that are judged to be endothelialised
Valve replacement or implantation of a cardiac device (e.g., pacemaker, implantable cardioverter-defibrillator)[31]
Use of intravenous drugs[7]
Recent vascular access (e.g., peripheral venous cannula, central venous catheter).[32]
fever/chills
Most common presenting feature. Older or immunocompromised patients may present atypically, without fever.[7] Fever may be low-grade in subacute IE.
cardiac murmur
Heart murmurs are found in up to 65% of patients with IE but the classic new or worsening cardiac murmur is rare.[7] Patients who develop new regurgitant murmurs are at increased risk of developing congestive heart failure.
night sweats, malaise, fatigue, anorexia, weight loss, myalgias
Non-specific constitutional symptoms
weakness
The nature of weakness can be constitutional or focal. Systemic emboli should be suspected if patients present with asymmetric weakness consistent with stroke.
arthralgias
May represent a constitutional symptom or could be secondary to septic emboli to the affected joint.
headache
May represent a constitutional symptom or could be secondary to septic emboli.
shortness of breath
Dyspnoea on exertion, orthopnoea, and paroxysmal nocturnal dyspnoea are features of heart failure.
uncommon
meningeal signs
Secondary to septic emboli.
Janeway lesions
Haemorrhagic, macular, painless plaques with a predilection for the palms and soles.[Figure caption and citation for the preceding image starts]: Janeway lesionsFrom the collection of Sanjay Sharma, St George’s University of London, UK; used with permission [Citation ends].
Osler nodes
Small, painful, nodular lesions usually found on the pads of the fingers or toes.[Figure caption and citation for the preceding image starts]: Osler nodeFrom the collection of Sanjay Sharma, St George’s University of London, UK; used with permission [Citation ends].
Roth spots
Oval, pale, retinal lesions surrounded by haemorrhage detected on fundoscopy.[Figure caption and citation for the preceding image starts]: Roth spotsFrom the collection of Sanjay Sharma, St George’s University of London, UK; used with permission [Citation ends].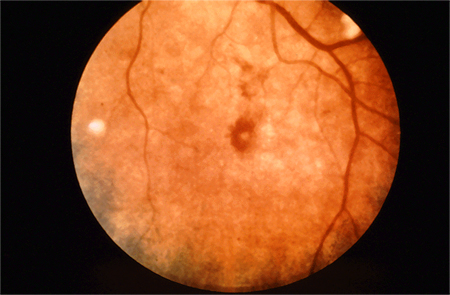
splinter haemorrhages
May be noted in the nails of the upper and lower extremities. They are non-specific.
Other diagnostic factors
uncommon
cutaneous infarcts
May be noted in distal extremities. They are non-specific.[Figure caption and citation for the preceding image starts]: Cutaneous infarctsFrom the collection of Sanjay Sharma, St George’s University of London, UK; used with permission [Citation ends].
chest pain
Can present with ischaemic chest pain secondary to decompensated heart failure due to acute valvular regurgitation or coronary artery emboli.
back pain
Could represent discitis from septic emboli.
palatal petechiae
May be present.
Use of this content is subject to our disclaimer