Case history
Case history
A 75-year-old man presents with an acute stroke including right-sided paralysis and impaired conscious level. Two days after admission, he notes cough and right-sided pleuritic chest pain. He is tachycardic, tachypnoeic, and has a fever of 38.8°C (102°F). His breath is foul smelling. Examination reveals poor cough with upper airway noises, decreased breath sounds, crackles, and dullness to percussion in the right lower lung field.
[Figure caption and citation for the preceding image starts]: Early ill-defined opacities of the right upper lobe above the minor fissure consistent with early changes of aspiration pneumoniaUsed with kind permission from Roy Hammond, MD [Citation ends].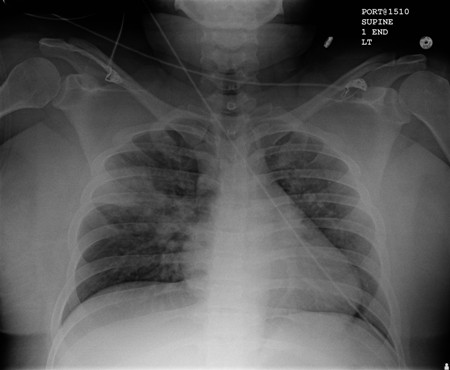 [Figure caption and citation for the preceding image starts]: Increased opacification of the right perihilar region and superior segment of the right lower and upper lobes consistent with worsening aspiration pneumoniaUsed with kind permission from Roy Hammond, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Increased opacification of the right perihilar region and superior segment of the right lower and upper lobes consistent with worsening aspiration pneumoniaUsed with kind permission from Roy Hammond, MD [Citation ends].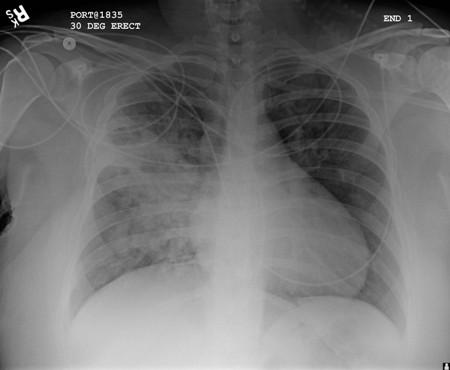
Other presentations
Aspiration pneumonia is more common in older individuals who have comorbid conditions that may lead to impaired conscious level. This population includes patients with swallowing dysfunction, disruption of the gastro-oesophageal junction, or anatomical abnormalities of the upper airway or digestive tract. Additionally, patients undergoing upper airway or endoscopic procedures are at risk. Any situation in which there is impaired conscious level and loss of airway protection mechanisms, such as seizure, places the patient at risk of aspiration. Nasogastric tube or percutaneous endoscopic gastrostomy provide no protection from colonised oral secretions.[8]
Use of this content is subject to our disclaimer