Investigations
1st investigations to order
serum electrolyte panel with glucose, urea, and creatinine
Test
Should be ordered in all patients with suspected hypernatraemia.
A serum sodium concentration >145 mmol/L confirms presence of hypernatraemia.[1] Severe hypernatraemia has variously been defined as a serum sodium concentration of >152 mmol/L, >155 mmol/L, or >160 mmol/L.[2][3][4] However, there is no consensus as to the exact level. Extremely high sodium levels occur in salt poisoning.
May reveal other electrolyte abnormalities, renal impairment, or uncontrolled diabetes mellitus. Some patients may have hypokalaemia or, more rarely, hypercalcaemia.
Patients with hypernatremia often have a high serum urea and/or creatinine level. The high urea level may worsen the hypernatraemia by causing an osmotic diuresis.[51][68]
Result
serum sodium >145 mmol/L; other parameters variable
urine osmolality
Test
Should be ordered in all patients with hypernatraemia, as it may help determine the underlying aetiology.
Urine osmolality ≤plasma osmolality (low; <150 mmol/kg): suggests diabetes insipidus.
Urine osmolality ≥plasma osmolality (high; >500 mmol/kg): suggests pure volume depletion not due to diabetes insipidus (e.g., gastrointestinal or insensible losses).
Urine osmolality not too different from plasma osmolality: suggests a renal concentrating defect most commonly due to renal failure, osmotic diuresis, and/or use of diuretics.
Can be variable in patients with iatrogenic hypernatraemia.
Result
<150 mmol/kg: diabetes insipidus; 200-500 mmol/kg: renal concentrating defect; >500 mmol/kg: pure volume depletion
serum osmolality
Test
Unlike hyponatraemia, hypernatraemia is always associated with serum hyperosmolality.
Result
>295 mmol/kg
urine electrolytes
Test
Should be ordered in patients with urinary losses to determine electrolyte-free water excretion.
Result
variable
urine flow rate
Test
Volume of urine excreted in a specific time period (e.g., over 30-60 minutes).
Should be ordered in patients with urinary losses to determine electrolyte-free water excretion.
Result
variable
electrolyte-free water excretion
Test
Should be calculated in patients with urinary losses.[Figure caption and citation for the preceding image starts]: Electrolyte-free water excretion formula. V = urine flow rate. UNa = urine concentration of sodium (mmol/L). UK = urine concentration of potassium (mmol/L). PNa = plasma concentration of sodium (mmol/L)Created by the BMJ Knowledge Centre [Citation ends].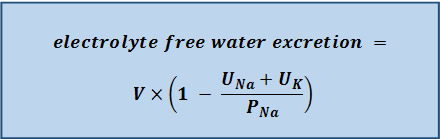
The electrolyte-free water excretion (also known as electrolyte-free water clearance) value indicates how much electrolyte-free water is being lost through the urine at any given time.[64][68][77] However, it does not provide a value for the total amount of free water needed to correct the hypernatraemia.[78]
Result
low (<0.5 L/day): suggests inadequate free water intake; high (≥1 L/day): suggests large free water losses; very high (>5 L/day): suggests diabetes insipidus
Investigations to consider
desmopressin challenge test
Test
Should be ordered in patients with suspected diabetes insipidus.
Differentiates between central and nephrogenic diabetes insipidus.
Patients are given a standard dose of desmopressin, and serum osmolality, urine osmolality, and urine volumes are measured hourly over a 4-hour period.
Patients with central diabetes insipidus respond to desmopressin with a reduction in urine output and increased urine osmolality. Patients with nephrogenic diabetes insipidus have little or no response.
Result
decreased urine output; increased urine osmolality (central diabetes insipidus)
serum arginine vasopressin (AVP) level
Test
May be useful to help distinguish central diabetes insipidus from nephrogenic diabetes insipidus.
Result
low (central diabetes insipidus)
MRI or CT brain
Test
Recommended in all patients with central diabetes insipidus to determine the underlying cause.
Result
may show pituitary tumour or other abnormalities
Serum creatine phosphokinase (CPK)
Test
May be helpful in evaluating the underlying cause, particularly hypernatraemia associated with rhabdomyolysis.
Result
elevated in hypernatraemia associated with rhabdomyolysis
Renal ultrasound
Test
May be helpful in evaluating the underlying cause, particularly to rule out obstructive uropathy in patients with renal disease.
Result
may show hydronephrosis in hypernatraemia associated with obstructive uropathy
Use of this content is subject to our disclaimer