History and exam
Key diagnostic factors
common
presence of risk factors
Key risk factors include non-metastatic malignancy (humoral hypercalcaemia), metastatic skeletal involvement (local osteolytic hypercalcaemia), and lymphoma (calcitriol [(1,25-dihydroxyvitamin D)]-mediated hypercalcaemia).
history of malignancy
Hypercalcaemia occurs in 20% to 30% of patients with cancer.[21][22] Cancer represents the most common aetiology of hypercalcaemia in the inpatient setting.[3] It can result from: humoral hypercalcaemia of malignancy (characterised by tumour secretion of parathyroid hormone-related peptide [PTHrP]); local osteolytic hypercalcaemia (characterised by local release of factors, including PTHrP, by bony metastases that promote osteoclast differentiation and function); calcitriol (1,25-dihydroxyvitamin D)-mediated hypercalcaemia (characterised by autonomous production of calcitriol [(1,25-dihydroxyvitamin D)] by lymphoma cells); and ectopic hyperparathyroidism (characterised by tumour production of parathyroid hormone), which is very rare.[21][5]
Other diagnostic factors
common
normal physical exam
Hypercalcaemia may not be associated with any specific physical examination findings.
poor skin turgor and/or dry mucous membranes
Signs of dehydration may be apparent on physical examination.
confusion
Hypercalcaemia may be associated with neuropsychiatric symptoms.
fatigue
Hypercalcaemia may be associated with neuropsychiatric symptoms.
constipation
Hypercalcaemia is associated with gastrointestinal symptoms.
loss of appetite
Hypercalcaemia is associated with gastrointestinal symptoms.
nausea
Hypercalcaemia is associated with gastrointestinal symptoms.
polyuria
Hypercalcaemia is associated with increased urinary excretion and dehydration by inducing nephrogenic diabetes insipidus.
polydipsia
Hypercalcaemia is associated with increased urinary excretion and dehydration.
bone pain
Hypercalcaemia is associated with bone pain.
Bone pain may be a feature of metastatic skeletal involvement.
uncommon
stupor
Hypercalcaemia may be associated with neuropsychiatric symptoms. Stupor is a non-specific symptom that may result from hypercalcaemia, but has numerous toxic/metabolic and neurological aetiologies that need to be considered.
coma
Hypercalcaemia may be associated with neuropsychiatric symptoms. Coma is a non-specific symptom that may result from hypercalcaemia, but has numerous toxic/metabolic and neurological aetiologies that need to be considered.
Risk factors
strong
non-metastatic malignancy
metastatic skeletal involvement
Local osteolytic hypercalcaemia occurs with disease complicated by widespread skeletal involvement.[1] Types of cancer include breast cancer and multiple myeloma.[1][5][10][Figure caption and citation for the preceding image starts]: CT chest showing compression fracture of multiple vertebral bodies in a child presenting with acute lymphoblastic leukaemia. Biochemistry showed hypercalcaemia with a suppressed parathyroid hormone levelSukumar SP, Balachandran K, Sahoo JP, et al. Acute lymphocytic leukaemia presenting as a metabolic bone disease. BMJ Case Reports 2013; doi:10.1136/bcr-2013-008758 [Citation ends].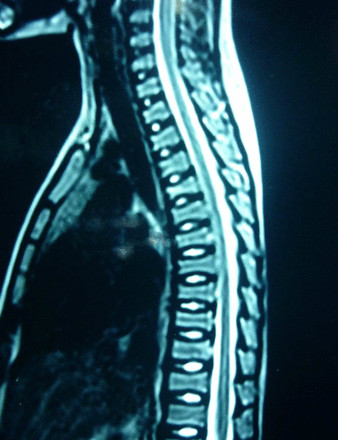 [Figure caption and citation for the preceding image starts]: Whole body planar images suggestive of skeletal infiltration in a child with acute lymphoblastic leukaemia showing areas of abnormal increased uptake. Biochemistry showed hypercalcaemia with a suppressed parathyroid hormone levelSukumar SP, Balachandran K, Sahoo JP, et al. Acute lymphocytic leukaemia presenting as a metabolic bone disease. BMJ Case Reports 2013; doi:10.1136/bcr-2013-008758 [Citation ends].
[Figure caption and citation for the preceding image starts]: Whole body planar images suggestive of skeletal infiltration in a child with acute lymphoblastic leukaemia showing areas of abnormal increased uptake. Biochemistry showed hypercalcaemia with a suppressed parathyroid hormone levelSukumar SP, Balachandran K, Sahoo JP, et al. Acute lymphocytic leukaemia presenting as a metabolic bone disease. BMJ Case Reports 2013; doi:10.1136/bcr-2013-008758 [Citation ends].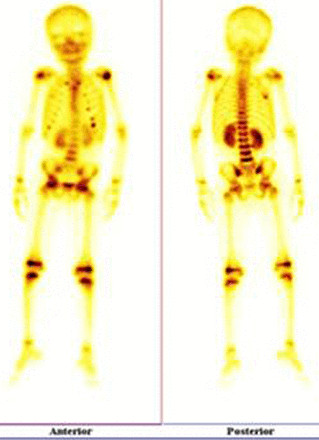
Use of this content is subject to our disclaimer