Aetiology
Breast cancer most often involves the glandular breast cells in the ducts or lobules. Men with breast cancer tend to present later than women; symptoms and diagnosis are the same.[7][8]
Benign breast masses
Fibroadenoma
The most common cause of breast mass. Fibroadenomas occur more commonly during the early reproductive years. Autopsy studies reveal these lesions in 9% to 10% of all women.[9] The exact cause of fibroadenomas is unknown, but their development is thought to be hormonally related.[10] Although these are benign lesions, some studies suggest that women diagnosed with fibroadenoma have approximately twice the risk of developing breast cancer relative to women without the lesions.[11] However, this is not supported by more recent data.[12]
Phyllodes tumour
Rare growths of the breast that can have benign or malignant characteristics.[13] They generally present as a rapidly growing, painless breast mass. Phyllodes tumours are sometimes difficult to distinguish histologically from fibroadenomas.[14][15] Increased cellularity, atypia, mitoses, and positive margins are often associated with an increased risk of local recurrence for Phyllodes tumours. Tumour size, necrosis, and stromal overgrowth are predictors of distant metastases. None of these, however, is a definitive marker of malignancy, and excision remains the mainstay of management.[13]
Fibrocystic breast
Fibrocystic breast is most commonly found in premenopausal and perimenopausal women.[16] The condition encompasses a spectrum of pathological changes: as well as cysts, it includes epithelial hyperplasia, apocrine metaplasia, and cystic dilation and fibrosis. Patients will sometimes present with a complaint of a discrete mass when they are actually detecting an area of normal nodularity associated with fibrocystic changes. Benign breast cysts are relatively uncommon in postmenopausal women not taking hormones.[17] Their presence in older women should raise the possibility of malignancy.
Cysts are characteristically mobile and have distinct borders on examination.
Cysts are sometimes tender and can fluctuate with the menstrual cycle.
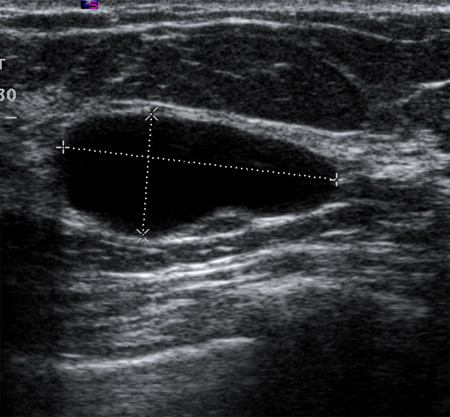
Simple cysts are completely anechoic, are distinct from the surrounding breast tissue on breast ultrasound, and are benign.[18][Figure caption and citation for the preceding image starts]: Ultrasonographic image of a simple cystCourtesy of Dr Lane Roland, University of Louisville; used with permission [Citation ends].
Complex cysts are associated with internal septations or debris, and should raise the suspicion of malignancy. National Comprehensive Cancer Network (NCCN) guidance recommends evaluation of these cysts by tissue biopsy.[19][Figure caption and citation for the preceding image starts]: Ultrasonographic image of a complex cystCourtesy of Dr Lane Roland, University of Louisville; used with permission [Citation ends].

Fat necrosis
Fat necrosis occurs secondary to injury of the breast. The source may be iatrogenic (e.g., breast biopsy, breast reduction or augmentation) or traumatic (e.g., seat belt injury to the breast).[20][21][22] Many women who present with fat necrosis have no recollection of breast trauma. Lesions present as hard, fixed masses and demonstrate acoustic shadowing on ultrasonography - characteristics suspicious for malignancy that mandate biopsy.
Breast papilloma
A bloody nipple discharge is typical of breast papilloma. This type of lesion can occasionally be detected as a mass within the breast. The growths often occur within the breast ducts (intraductal papillomas). These lesions are typically benign, but they can be associated with histological findings of atypia, papillary ductal carcinoma in situ (DCIS), or invasive papillary cancer.[Figure caption and citation for the preceding image starts]: Ductogram demonstrating multiple intraductal papillomasCourtesy of Dr Nancy Pile, University of Louisville; used with permission [Citation ends].
Breast abscess
Breast abscesses typically occur in women who are breastfeeding. They are thought to result from ruptured sub-areolar ducts that leak into the periductal space. Abscess must be differentiated from inflammatory breast cancer (which, paradoxically, does not present as a breast mass).[Figure caption and citation for the preceding image starts]: Ultrasonographic image of skin thickening in patient with inflammatory breast cancerCourtesy of Dr Nancy Pile, University of Louisville; used with permission [Citation ends].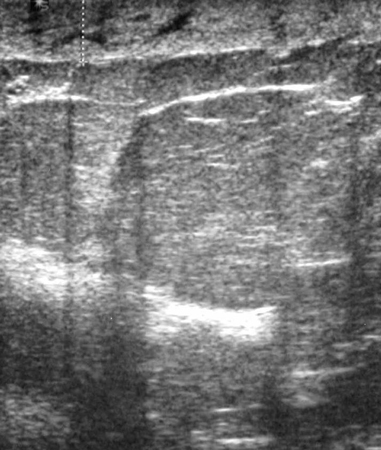
Adenomas
Adenomas are similar to fibroadenomas, but differ slightly in their histology. Many are tubular adenomas, which present as well-demarcated growths in young women. Lactating adenomas may occur during pregnancy or the postpartum period.[23]
Malignant breast masses
Invasive breast carcinoma may present as a palpable (symptomatic) or non-palpable mass, identified on screening imaging (e.g. mammography or MRI in women undergoing high-risk screening). The most common histological subtype is invasive ductal carcinoma, which arises from the ducts of the breast. Some of these tumours (e.g., invasive lobular carcinomas) may present as a palpable mass, due to the single file pattern of cellular spread characteristic of this histological subtype of malignancy, without related imaging findings.[24]
Other malignant tumour subtypes that are classified as invasive breast carcinoma include tubular carcinoma, mucinous or colloid carcinoma, papillary carcinoma, and medullary carcinoma. All are diagnosed and treated in the same way.
Ductal carcinoma in situ (DCIS) is a proliferation of malignant-appearing epithelial cells that have not penetrated the basement membrane. The terminal duct lobular unit is the origin of most lesions. Most cases are diagnosed on mammography; however, 10% of DCIS lesions present as palpable masses.[25]
Cancer metastatic to the breast is exceedingly rare, comprising 0.5% to 2.0% of metastases from primary cancers.[26] Melanoma, ovarian carcinoma, lung cancer, and lymphoma have been implicated.[27][28]
See Primary invasive breast cancer, Breast cancer in situ, and Metastatic breast cancer.
Premalignant breast lesions
Both atypical ductal hyperplasia (ADH) and atypical lobular hyperplasia (ALH) are associated with an increased risk of breast cancer. Core needle biopsy findings of ADH mandate further sampling with vacuum-assisted excision (VAE) or surgical excision of the breast mass, as these lesions are upstaged to ductal carcinoma in situ (DCIS) in nearly 15% of cases.[29][30]
Lobular carcinoma in situ (LCIS) is an incidental finding that is a marker of increased risk for breast cancer.[24] It may be associated with palpable lesions. LCIS has been classified into 2 subtypes:
A classical subtype that is a marker of increased risk in either breast. Further sampling with surgical excision or VAE is recommended, as the risk of upgrade to invasive cancer is up to 27%.[29][Figure caption and citation for the preceding image starts]: Histopathology of classic lobular carcinoma in situ (LCIS)Courtesy of Dr Sunati Sahoo, University of Louisville; used with permission [Citation ends].

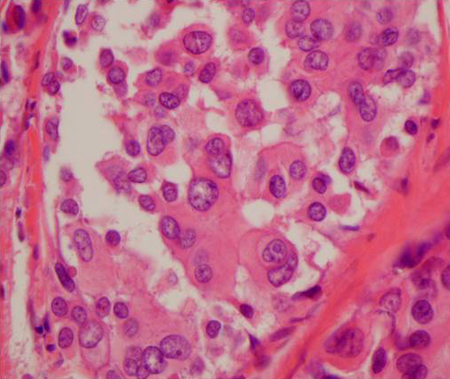
A pleomorphic subtype that behaves more like DCIS, in that it is thought to be a precursor of invasive disease and needs to be treated in a similar way.[Figure caption and citation for the preceding image starts]: Histopathology of pleomorphic lobular carcinoma in situ (LCIS)Courtesy of Dr Sunati Sahoo, University of Louisville; used with permission [Citation ends].
Use of this content is subject to our disclaimer