Article Text

Abstract
Objectives Reliable and valid information on burden of road traffic injuries (RTIs) is essential for short-term and long-term planning. We designed the present study to describe the levels and trends of burden of RTIs in Iran from 1990 to 2019.
Methods This is an observational epidemiological study. We used the Global Burden of Disease (GBD) 2019 estimates to report RTIs incidence, prevalence, mortality and disability-adjusted life-years (DALYs) by sex, age group and road user category in Iran and each of the 31 provinces from 1990 to 2019.
Results Age-standardised incidence, prevalence, death and DALY rates of RTIs decreased by 31.7% (95% uncertainty interval (UI): 29.4 to 33.9), 34.9% (33.8 to 36.0), 57.7% (48.1 to 62.3) and 60.1% (51.7 to 65.2), respectively between 1990 and 2019. The 2019 age-standardised DALY rates varied from smallest value in Tehran 303.8 (216.9 to 667.2) per 100 000 to largest value in Sistan-Baluchistan 2286.8 (1978.1 to 2627.9) per 100 000. The burden of RTIs was mainly related to injuries sustained by drivers or passengers of motorised vehicles with three or more wheels and pedestrians’ injuries, mostly affected males aged 15–29 years and individuals aged ≥70 years.
Conclusion The reducing trend in the burden of RTIs in Iran possibly reflects the effectiveness of the intervention programmes. However, with regard to the Sustainable Development Goals the burden is still at an alarming level. Further reductions are necessary for specific road user groups such as adolescent and adult male drivers or passengers of motorised vehicles, also pedestrians aged ≥70 years.
- mortality
- disability
- burden of disease
- descriptive epidemiology
- public health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Road traffic injuries (RTIs) are the second cause of morbidity and mortality in Iran.
No comprehensive study on RTIs has been developed in Iran at the national and subnational levels over the past 30 years.
WHAT THIS STUDY ADDS
To our best knowledge, this study is the first one that represents burden of RTIs in Iran at national and subnational levels using the Global Burden of Disease (GBD) 2019 reports.
Burden of RTIs in Iran showed 61.1% decrease from 1990 to 2019.
The current study allows comparisons of RTIs statistics at global, national and subnational levels and offers a unique perspective of reporting both fatal and non-fatal consequences of RTIs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Reduction in burden of RTIs from 1990 to 2019, possibly reflecting the effectiveness of the traffic intervention programmes.
Neglecting vulnerable road users is obvious that emphasises road safety measures in Iran should also be designed for specific road user groups such as adolescent and adult male drivers or passengers of motorised vehicles with three or more wheels, also pedestrians aged ≥70 years.
The GBD is a vital resource for researchers, policymakers and practitioners that can be used to identify and prioritise action areas for prevention of RTIs at national and subnational levels.
Introduction
Road traffic injuries (RTIs) are the eighth leading cause of death for people of all ages and the first cause of death for children and young adults aged 5–29 years worldwide. WHO suggests improving access to reliable and comprehensive data for monitoring the implementation and progress of road safety strategies. Halving the number of global deaths and injuries from RTIs by 2020 was one of the Sustainable Development Goals (SDGs) adopted by all member states of the United Nations. However, according to the WHO report, most of the countries have not achieved this goal.1
The age-standardised mortality rate due to RTIs in Iran was 59.87 (95% uncertainty interval (UI): 50.33 to 71.35) and 34.82 (95% UI: 28.97 to 42.3) per 100 000 in 1990 and 2016, respectively. RTIs are the second leading cause of death and disability-adjusted life-years (DALYs) in Iran. The age-standardised mortality rate due to RTIs is expected to reach 17.95 (95% UI: 9.98 to 30.82) per 100 000 in 2030.2 On the other hand, years of life lost (YLLs) due to premature mortality of RTIs are higher in Iran compared with most parts of the world.3 Additionally, these injuries account for about 5% of Gross Domestic Product (GDP).4
Since 2004, several interventions have been developed to reduce RTIs in Iran. ‘Pupil Liaisons Policy’ or ‘Police Supporters’ Plan’, increase in traffic speeding ticket price, law implementation (mandatory using safety belts and helmets, provisional driving license for drivers who are under 23 years old, mandatory installation of antilock braking system and airbags), educational programme campaigns using the national broadcasting services, increase in number of ambulances (seven times) and Emergency Medical Services (EMS) posts (four times), new air emergency bases establishment, a significant reduction in ambulance transfer time and providing full medical insurance coverage have been some of the successful interventions in Iran. Assessing the impact of RTIs interventions is critical to support future decision making.
Evaluation of some interventions in Iran yielded the following results: the number of deaths due to RTIs after the implementation of safety belts law decreased by 3.3%, the number of driving injuries decreased by 7% among drivers under the age of 23 years and the number of traffic law violations showed a decrease of 17.9% after implementation of ‘Police Supporters’ Plan’. Overall, all these interventions reduced the number of deaths due to RTIs from 38.2 per 100 000 in 2004 to 31.8 per 100 000 persons in 2008.5–8
To the best of our knowledge, there is not a reliable and comprehensive study on burden of RTIs in Iran at the national and provincial levels over the past decades.9 This study aims to describe long-term patterns of fatalities due to RTIs, to define the distribution of injuries among different road user groups and to identify population at-risk from 1990 to 2019.
We analysed mortality and DALYs attributed to RTIs in Iran and its provinces using the Global Burden of Disease (GBD) 2019 study. Burdens were reported in absolute numbers and age-standardised rates per 100 000 populations by sex, age group and type of road users with 95% UIs. We also reported percentage changes in mortality and DALYs between 1990 and 2019.
Methods
Design
The present study is an observational epidemiological study. We considered results using disaggregated incidence, prevalence, deaths, years lived with disability (YLDs), YLLs and DALYs of RTIs in Iran by age, sex and category of road user during 1990–2019. Descriptive statistics such as rates, percentages and numbers were reported. Similar analyses were conducted for each of 31 provinces across the country.
Data source
GBD 2019 provided estimates of the burden of 369 diseases and injuries and 87 risk factors for 204 countries and territories from 1990 to 2019, with subnational estimates for 21 countries, including Iran. The GBD study followed a systematic and scientific approach to provide adequate evidence on the extent of human health outcomes as well as its trends.10 The detailed estimation framework of GBD 2019 has been discussed previously.10–14
All data sources used in our analysis and related code can be found on the Global Health Data Exchange. GBD 2019 used several databases for RTIs in Iran. The data for national and subnational estimates of RTIs in Iran were retrieved from various sources, including national death registration system, national forensic medicine system, hospital data sample and Iran’s Demographic and Health Survey.15 16
In GBD study, deaths with uninformative, so-called garbage codes are redistributed to the most important causes of death. Also, data are corrected in terms of misclassification, miscoding and under-reporting.17 Comparability as well as the quality of death data in GBD has been done in several ways.12 14
The injury-related death record in this study was categorised based on the GBD cause of death categorisation for road injury18–21 (table 1).
Cause of death categorisation for road injuries according to the Global Burden of Disease study 2019
Statistical modelling
The target population in this study was divided into 13 age groups including infants (under 1 year old), children 1–4 years old, 9 other age groups from 5 years to 49 years with intervals of 5 years, age group 50–69 years old and one age group over 70 years (+70 years).
Cause-specific death rates and cause fractions were calculated using the Cause of Death Ensemble model and Spatiotemporal Gaussian process regression. All rates were adjusted using the direct age-standardised method.
To calculate the YLLs, deaths from RTIs were multiplied by standard life expectancy at each age using the standard life table. A Bayesian meta-regression modelling tool, DisMod-MR 2.1, was used to ensure the consistency between incidence, prevalence, excess mortality and cause-specific mortality. To calculate the YLDs, prevalence estimates of non-fatal RTIs were multiplied by disability weights of mutually exclusive sequelae of RTIs. A disability weight reflects the magnitude of the health loss associated with an outcome and ranges between 0 (meaning full health) and 1 (equal to death). The prevalence of RTIs was also estimated from the incidence models that use the estimated duration of each injury. To calculate the DALY, the premature death values YLLs and YLDs were added together. DALYs of RTIs mean the loss of healthy living due to RTIs and were calculated by measuring the difference between the current state of health and the ideal situation that anyone of any age can spend in that ideal position. In this study, point estimation and 95% UI were presented for all indices. The UI represents a parametric change, and uncertainty considers potential biases in information, heterogeneity in information sources, data generation stages and model selection in the estimation process. We present 95% UIs for every metric based on the 25th and 975th ordered values of 1000 draws of the posterior distribution.10
Data coding was performed using Stata (V.11) and all graphs were created by R statistical software V.3.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
National overview of burden of RTIs
In 2019, RTIs in Iran accounted 21 122.0 (95% UI: 18 110.0 to 24 648.3) deaths, of which 77.2% and 22.8% occurred in males and females, respectively. In the same year, RTI was the third leading cause of death (5.4% of all deaths; 95% UI: 4.62% to 6.27%) in Iran.
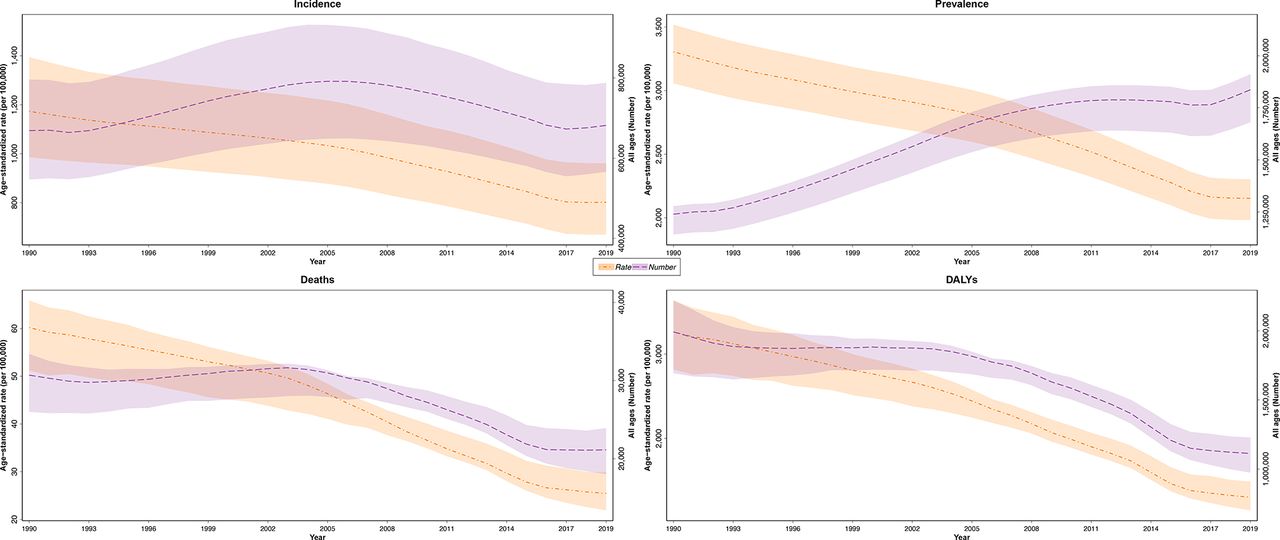
The number of deaths due to RTIs increased from 1990 to 2003, followed by a decreasing trend through 2017, but the trend was upwards from 2017 to 2019. The prevalence of RTIs increased from 1990 to 2019 except for a 3-year period (2015–2017) that remained relatively stable. However, age-standardised incidence, prevalence, death and DALY rates due to RTIs declined over the study period (figure 1 and online supplemental figure 1A).
Supplemental material

Time trend of all ages number and age-standardised rate of road traffic injuries incidence, prevalence, deaths and DALYs for both sexes, 1990–2019, Iran. Shaded sections indicate 95% uncertainty intervals. DALY, disability-adjusted life-year.
The age standardised mortality rate due to RTIs decreased from 60.2 (95% UI: 51.2 to 65.9) per 100 000 in 1990 to 25.4 (95% UI: 21.9 to 29.9) per 100 000 population in 2019.
Despite the similarity of the trend of ASMR in males and females from 1990 to 2019, the decrease was more in females (62.6%) than in males (55.7%). In addition, the national male-to-female ASMR ratio changed from 2.7 to 3.2 over the study period (table 2).
Age-standardised incidence, prevalence and burden of road traffic injuries and subcauses per 100 000 and per cent change, by sex from 1990 to 2019, Iran
All road users experienced decrease in ASMR due to RTIs during the study period. The only increase in ASMR due to RTIs (10.9%) was seen among males from ‘other road injuries’. Males from ‘other road injuries’ also showed an increase in age-standardised RTIs incidence (7.8%) and prevalence (10.3%) from 1990 to 2019.
The highest decrease in ASMR occurred in injuries sustained by drivers or passengers of motorised vehicles with three or more wheels with per cent changes of 59.8% followed by pedestrians (56%), motorcyclists (55.8%), bicyclists (39.8%) and ‘other road injuries’ (14.2%), respectively.
In 2019, ASMR due to RTIs in males and females was 38.5 (95% UI: 32.8 to 46.8) and 12.0 (95% UI: 10.3 to 13.0) per 100 000, respectively. In 2019, injuries sustained by drivers or passengers of motorised vehicles with three or more wheels had the highest ASMR of 12.9 (95% UI: 2.3 to 4.8) per 100 000 population, followed by pedestrians 8.8 (95% UI: 6.8 to 10.6), motorcyclists 3.2 (95% UI: 2.3 to 4.8) and bicyclists 0.4 (95% UI: 0.3 to 0.7) (table 2 and online supplemental figure S1).
Years of life lost: premature death
The rate of age-standardised YLL due to RTIs decreased from 3063.5 (95% UI: 2615.8 to 3419.8) per 100 000 in 1990 to 1184.7 (95% UI: 1031.7 to 1370.1) per 100 000 population in 2019. Despite the similarity of the trend of age-standardised YLL in males and females from 1990 to 2019, the decrease was more in females (69.2%) than in males (58%).
From 1990 to 2019, all road user categories showed decreases in age-standardised YLL rate, however the highest reduction related to injuries sustained by drivers or passengers of motorised vehicles with three or more wheels at 62.6%.
In 2019, the rate of premature death from RTIs was higher in males (1803.7 per 100 000; 95% UI: 1562.5 to 2136.1) than in females (546.3 per 100 000; 95% UI: 474.7 to 596.4).
In the same year, the highest rate of age-standardised YLL (605.8 per 100 000; 95% UI: 512.1 to 758.5) was related to injuries sustained by drivers or passengers of motorised vehicles with three or more wheels (table 2 and online supplemental figure S3).
Years lived with disability
The rate of age-standardised YLD due to RTIs decreased from 199.1 (95% UI: 144.6 to 264.1) per 100 000 in 1990 to 117.4 (95% UI: 83.5 to 157.9) per 100 000 population in 2019.
Despite the similarity of the trend of age-standardised YLD in males and females from 1990 to 2019, the decrease was more in females (45.1%) than in males (38.2%).
From 1990 to 2019, drivers or passengers of motorised vehicles with three or more wheels, pedestrians, motorcyclists, bicyclists and ‘other road injuries’ in both sex combined showed a decrease in age-standardised YLDs due to RTIs by 42.9%, 41.5%, 48.3%, 7.6% and 4.1%, respectively. The only exception was related to males from ‘other road injuries’ that showed a 6.8% increase in age-standardised YLDs.
In 2019, RTIs resulted in 149.6 (95% UI: 106.0 to 201.9) and 84.5 (95% UI: 60.3 to 112.4) YLDs per 100 000 for males and females, respectively. In the same year, the highest age-standardised YLDs 34.3 (95% UI: 23.5 to 47) per 100 000 were related to pedestrian road injuries (table 2 and online supplemental figure S4).
Disability-adjusted life-years
The rate of age-standardised DALY due to RTIs decreased from 3262.5 (95% UI: 2815.5 to 3635.4) per 100 000 in 1990 to 1302.1 (95% UI: 1147.4 to 1488.3) per 100 000 population in 2019. This reduction was more in females (67.3%) than in males (57.0%).
From 1990 to 2019, DALYs due to RTIs decreased in all road user categories. The highest reduction in DALYs rate occurred in injuries sustained by drivers or passengers of motorised vehicles with three or more wheels at 61.8% (table 2 and online supplemental figure S2).

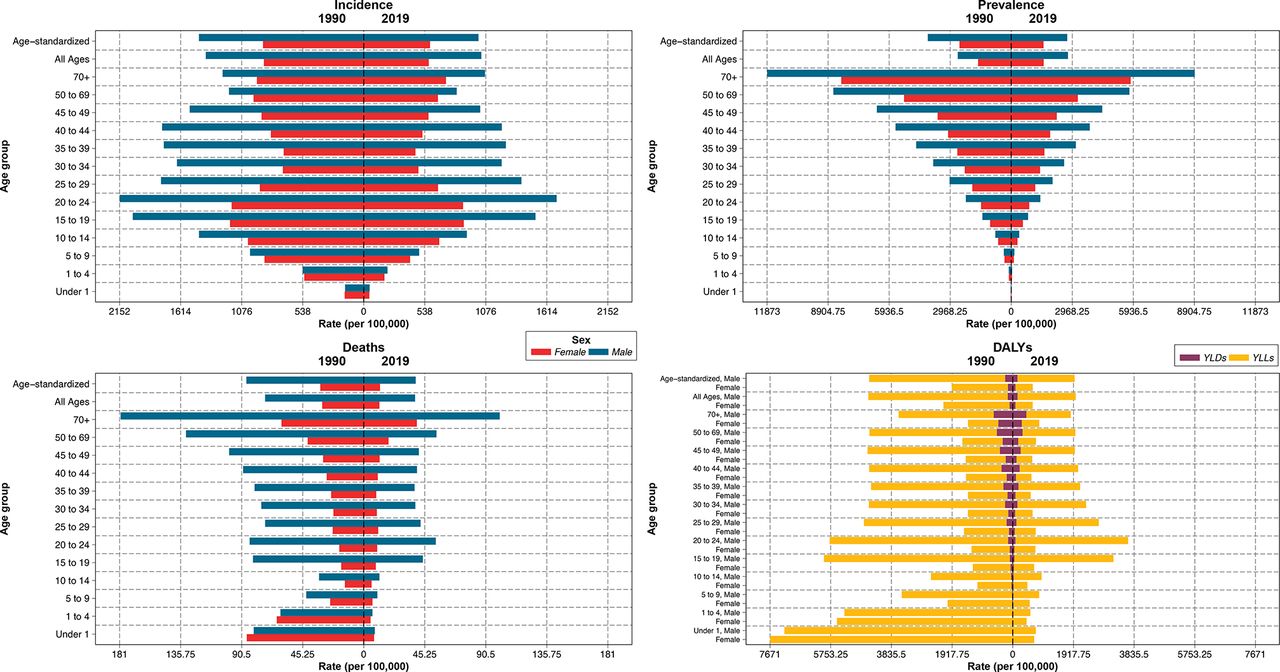
Incidence, prevalence, death and disability-adjusted life-years (DALYs) rate per 100 000 due to road traffic injuries by sex, age group, 1990 vs 2019, Iran. YLD, years lived with disability; YLL, years of life lost.
In 2019, RTI was the second leading cause of DALYs (5.63% of all DALYs; 95% UI: 4.83% to 6.58%) in Iran. In this year, RTIs resulted in 1953.3 (95% UI: 1712.5 to 2284.3) and 630.8 (95% UI: 557.5 to 689.5) DALYs per 100 000 for males and females, respectively (3.1-fold difference).
In 2019, the highest age-standardised DALYs (644.6 per 100 000; 95% UI: 550.8 to 792.5) were related to injuries sustained by drivers or passengers of motorised vehicles with three or more wheels.
In 2019, The YLL component of DALYs due to RTIs in injuries sustained by drivers or passengers of motorised vehicles with three or more wheels, pedestrians, motorcyclists, cyclists and ‘other road injuries’ was 94.0%, 91.7%, 88.7%, 52.2% and 49.2%, respectively.
The current study showed that YLLs were accountable for 91% of total DALYs due to RTIs in 2019 compared with 94% in 1990.
Age trend of RTIs
From 1990 to 2019, age-standardised incidence, prevalence, death and DALY rates due to RTIs decreased in all age groups of both sexes (figure 2).
This figure highlights that the burden of RTIs for males was higher than for females in all age groups in 2019.
In 2019, the highest prevalence, deaths and YLDs rates due to RTIs occurred in individuals aged ≥70 years. However, the highest incidence, YLL and DALY rates belonged to people aged 15–24 years.
In 2019, in males and females, the highest ASMR due to RTIs occurred in people aged ≥70 years; also pedestrians were the predominant cause of ASMR due to RTIs in individuals aged ≥70 years.
Among males, the highest DALYs due to RTIs belonged to people aged 20–24 years in 2019. Injuries sustained by drivers or passengers of motorised vehicles with three or more wheels were the prevailing cause of RTIs DALYs in males aged 20–24 years.
Among females, the highest DALYs due to RTIs was related to people aged ≥70 years in 2019. Pedestrians were the predominant cause of DALYs due to RTIs in females aged ≥70 years, however, injuries sustained by drivers or passengers of motorised vehicles with three or more wheels were the main cause of DALYs in females aged 20–29 years (online supplemental figure 2A–E).
Subnational overview of burden of RTIs
As depicted in figure 3, there was a wide variation in age-standardised rates of incidence, prevalence, death and DALYs among provinces in Iran from 1990 to 2019. Lower burden of RTIs was observed in all provinces in 2019 compared with 1990 (online supplemental figure 3A). In 1990, the highest age-standardised incidence and prevalence rates due to RTIs were identified in the North and South provinces, however, the highest age-standardised death and DALY rates belonged to the Eastern part of the country which includes the largest provinces in terms of area. In 2019, age-standardised incidence, prevalence, death and DALY rates due to RTIs were the highest in South of Iran including the first three large provinces.

Provincial distribution of age-standardised incidence, prevalence, death and disability-adjusted life-years (DALYs) rate due to road traffic injuries per 100 000 in Iran, both sexes, 1990 vs 2019.
In 1990, the highest ASMR of RTIs occurred in Khorasan-e-Razavi 99.3 (95% UI: 71.2 to 122.2) per 100 000 that was 9.8 times of the lowest rate observed in Tehran (10.1 per 100 000; 95% UI: 6.5 to 24.7). In 2019, the provinces with the highest and lowest ASMR were Sistan-Baluchistan 44.2 (95% UI: 37.2 to 51.8) per 100 000 and Tehran 4.6 (95% UI: 2.9 to 12.7) per 100 000, respectively (9.6-fold difference) (figure 4). Also Sistan-Baluchistan and Tehran represented the highest and lowest age-standardised DALY rates, respectively (7.5-fold difference) in 2019 (online supplemental figure 4A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ranking of age-standardised death rates due to road traffic injuries per 100 000, by province, Iran, 1990 vs 2019.
From 1990 to 2019, the percentage of change in new cases for RTIs varied widely between the provinces, including a reduction of 25.1% in Hamadan and an increase of 66.3% in Sistan-Baluchistan (online supplemental table 2A). A huge variation in age-standardised burden of RTIs among provinces was seen by road user categories (online supplemental file 3).
Supplemental material
Supplemental material
Discussion
Using up-to-date data from the GBD 2019, to our knowledge this is the first study on national and subnational estimates for burden of RTIs in Iran and to explore the level and trend of burden of RTIs between 1990 and 2019. As measured by changes in four indicators (age-standardised incidence, prevalence, death and DALYs per 100 000), we found that despite national and subnational increase in RTIs prevalence between 1990 and 2019, burden of RTIs decreased over the same time period. One exception to this trend occurred in the last 3 years that the burden remained relatively constant. This finding was almost consistent with the previous studies in Iran3 9 22, Mexico23, China24 and India25. Declining in burden of RTIs despite increase in its prevalence could be partly explained by decreased fatality rates due to broadly increasing access to and utilisation of motorised transport that shifted the type of vehicles (eg, from bicycles and motorcycles to more safer vehicles such as automobiles and public transport) being used. It seems that countermeasures that reduced the severity of RTIs resulted in decreased mortality rate which likely represented progress in road safety initiatives.26
Despite a significant decline in the RTIs DALY rate over three decades in Iran, DALYs rate for RTIs in 2019 was about 1.5 times higher than the global average. In addition, RTIs age-standardised incidence, YLL and YLD rates per 100 000 in Iran showed significantly higher values than global ones.27 In another study, the observed rates of DALYs due to RTIs were significantly higher than expected levels in Iran, Oman, United Arab Emirates and Russia. Conversely, observed RTIs DALYs rates in Qatar, Turkey and Kuwait were lower. This study emphasised the difference in terms of DALYs caused to RTIs in similar sociodemographic statuses and the importance of formulating prevention policies according to specific needs of each country. However, RTIs do not follow this pattern proportionally, which suggests the effects of multiple underlying mechanisms such as health system performance and geoepidemiological characteristics.27 28
Our study showed that the death rate due to RTIs in Iran decreased slightly over the recent three decades. Therefore, it seems highly unlikely that the country achieves the SDG target (50% reduction in the number of deaths and injuries from RTIs) by 2030.2 9 Lack of achievement of the SDG targets in RTIs in Iran indicates the existing challenges related to governance, human resources and capital investment in equipment and infrastructure and need for more effective measures.13 29
Previous studies showed that among 13 implemented interventions aimed to reduce RTIs the following three were the most effective interventions: using safety belts and helmets by drivers, pupil liaisons and speed limit laws.5 To minimise the risk of the postinjury phase, the EMS capacity was also improved in terms of technology, equipment and operation. This intervention declined mortality due to road injuries by 95% and reduced ‘on-scene’ and ‘transport’ time.7
With regard to SDG targets, the national action plan for non-communicable diseases prevention and control in Iran was developed in 2015. A specific objective of the plan was a 20% reduction in road traffic deaths by 2025. In addition, this action plan directly addressed alcohol use as one of the behavioural risk factors of RTIs.30
Consistent with other studies, RTIs were responsible for a higher proportion of the burden in males compared with females.1 22 27 This could be partly due to the fact that males typically drive more frequent and involve in high-risk behaviour more than females.3 31 Other studies reported higher death and DALY rates of RTIs in males may be associated with distances they travel, mode of transportation, road type and as a consequence of their violation of traffic laws.32 33
Such findings highlight the importance of considering gender differences when developing road injury prevention interventions. However, this need has not been taken into account appropriately. Further research in gender differences in road traffic crashes would be advisable.
From 1990 to 2019, the death and DALY rates due to RTIs decreased in all age groups. In 2019, in males and females, the highest age-standardised prevalence, death and YLD rates due to RTIs occurred in people aged ≥70 years. However, the highest incidence, YLL and DALY rates belonged to age group of 15–24 years old.
Consistent with the previous studies, higher mortality rate in the individuals aged ≥70 years can be explained by high frailty, high severity of injuries, low physical endurance and cognitive abilities. However, the role of the other two components (ie, exposure and injuryrisk) is not very clear.34 35
According to our study, the highest DALY rates in males and females were related to 15–24 age groups. This is comparable with other studies that showed RTIs accounted for an increasing proportion of the burden, especially among economically productive age groups. Moreover, adolescence is a developmental transition point from childhood to adulthood for injury risk. This can be due to factors such as increasing the level of self-reliance and increasing the level of risk taking.22 34 36
Our findings indicated a need to revise policies and intervention programmes for age-specific groups to decrease the burden of RTIs. For example, enforcing speed limits, preventing drinking and driving and creating public transport infrastructure are interventions that all age groups will take advantage. There are some age-specific interventions such as designing streets and traffic signs according to the needs of children, adolescents and elderly people. Meanwhile, children under the age of 15 years need educational interventions targeting requirements of safe travel and learning traffic rules in schools.35 37
Our study showed the trends of ASMR were decreasing in all road users except for ‘other road injuries’ over the study period. Hence, there is a need for more attention in this category.24
According to our results, in both sexes combined, the highest percentage of death due to RTIs belonged to the drivers or passengers of motorised vehicles with three or more wheels, followed by pedestrians, motorcyclist, cyclists and ‘other road injuries’. However, the proportion of pedestrian injuries by road vehicles substantially increased over the study period. Pedestrian injuries also were the most prevalent cause of death due to RTIs in the elderly. However, the most prevalent cause of death in adults was drivers or passengers of motorised vehicles with three or more wheels. The patterns of road user categories involved in road traffic crashes were consistent with previous researches and Eastern Mediterranean Region reports,22 38 however, differed from the global pattern. Comparing the proportion of deaths caused by RTIs in Iran and in the world showed more impact of drivers or passengers of three-or-more-wheeled motorised vehicles in Iran (51.5% vs 37.4%). In any case, vulnerable road users accounted for almost half of the deaths (48.5%) due to RTIs in Iran. Neglecting the vulnerable road users in the planning, designing and operation of roads and in vehicle design is prevalent in Iran and is also seen in many low-income and middle-income countries.1 The reasons may be partly related to the increased number of motorised vehicles (4.5 times increase from 2001 to 2014 in Iran) without using safety devices. Iran is the 16th largest car producer in the world. However, a report proving the compliance of passenger vehicles with safety regulations such as frontal impact, electronic stability control and pedestrian protection is not available. Overall, it seems although the successful interventions led to a reduction in road traffic deaths in Iran, unsafe vehicles increased the number of deaths. Additionally, traffic mix and unsafe infrastructures on the roads resulted in increased exposure without attention to the needs of vulnerable road users.9 38 To the best of our knowledge, there is not a specific RTI prevention policy targeting pedestrians in Iran, such as safer walking spaces.9
The incidence, prevalence, death and DALY rates for RTIs varied substantially between the provinces of Iran; however, the leading cause of RTIs was related to drivers or passengers of motorised vehicles with three or more wheels and the mortality rate in males was significantly higher than in females for all provinces. The lowest and the highest burden of RTIs belonged to Tehran and Sistan-Baluchistan provinces, respectively (9.6-fold difference). Similarly, other studies reported considerable heterogeneity in RTIs death rate across provinces in Iran.39 40 Inequalities within the country regarding burden of RTIs has been also reported in other countries.24 25 Disparities may be due to factors such as: geographical extent of provinces resulted in increased length of communication roads and poor access to rescue and relief centres, existence of two-way roads without standards, demographic structure, proportion of road users, safety of vehicles, different life styles, GDP, education level, high-risk behaviours related to mobility, level of economic activities, curved roads, mountain, river, tunnel and elevated lands. Some studies have also reported that high population density causes milder injuries and fewer deaths through slowing down the vehicles.24 40 Determining the trends and variations among the provinces is necessary to prioritise evidence-based, province-specific interventions.
Strengths and limitations
The main strength of this study is that it allows comparisons between the status of RTIs at global, national and subnational levels using the available data. It also offers a unique perspective that combines the fatal and non-fatal consequences of RTIs.
Our study, as a part of the GBD study, has some limitations.10 22 The rate of injuries and deaths due to RTI in Iran is influenced by the available data. Lack and/or dispersion of data leads to more reliance on modelling trends to estimate of causes of death, covariates and data of surrounding countries. The YLLs were accounted for >90% of DALYs, so burden estimates are more sensitive to the analysis of the cause of RTI deaths.9 Point estimates with large UIs in the results mean that we need to be careful when using these results in practice. Another limitation is that only one disability was used in the YLDs estimation process and the burden of other disabilities was not taken into account.
Conclusion
These data highlight a downward trend in burden of RTIs in Iran over the study period, possibly reflecting the effectiveness of interventions. This is a promising finding. Further reductions should therefore still be addressed by reinforcing the effective interventions already existing and implementing new interventions with respect to specific groups such as adolescent and adult male drivers/passengers of motorised vehicles, also pedestrians aged ≥70 years in high burden areas. An accurate understanding of these patterns, in addition to population risk metrics, requires more studies to determine exposure risk. If the trends reported in our study continue in the current pattern, it is unlikely that Iran and its provinces achieve the SDG 2020 target in 2020 or even in 2030.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank Professor Farshad Farzadfar in Non-Communicable Diseases Research Centre, Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences for recommendations and supporting this study. We also appreciate Dr Mohammadreza Pakseresht epidemiologist in University of Alberta for his valuable comments and edits.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Osteoporosis Research Center, Endocrinology and Metabolism Clinical Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors MRST, AO and ADT designed the study and oversaw research. SSM, PS and HF led the statistical analysis, and prepared results. MHE, IS and MRK contributed to study design and updated the manuscript. MRST wrote the first and final draft of the manuscript. ADT had primary responsibility for final content. All authors reviewed the final manuscript and approved of it. ADT is responsible for the overall content as guarantor.
Funding This paper is part of a PhD dissertation in 'Health in Emergencies and Disasters', which was financially supported by Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.