Differentials
Common
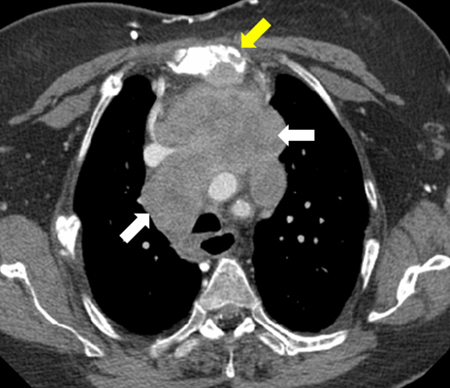
Thoracic aortic aneurysm
History
often asymptomatic, may present with chest or back pain; sudden-onset chest or back pain with associated hypotension and shock may be caused by aneurysm dissection or rupture; compression of adjacent structures may cause dysphagia or dyspnea; vascular compromise may lead to anginal symptoms, orthopnea, and peripheral edema; may have associated history of Marfan syndrome
Exam
signs of heart failure (elevated venous pressure, peripheral edema, respiratory distress); signs of aortic insufficiency (diastolic murmur, collapsing pulse); signs of aneurysm dissection or rupture (hypotension and shock, weak or unequal peripheral extremity pulses); associated signs of Marfan syndrome (arm span exceeding height, arachnodactyly, joint hypermobility)
1st investigation
- CT angiogram of chest:
detects thoracic aortic aneurysm, and determines its size, indicates if evidence of dissection or contained rupture
More
Other investigations
- CXR:
widened mediastinum silhouette, enlarged aortic knob
More - transesophageal echocardiography:
assess size, location of aneurysm, and the presence of a dissection; assess coexisting aortic valvular abnormalities
More - MRI:
detects thoracic aortic aneurysm and determines its size; not used in the acute setting
More
Non-Hodgkin lymphoma
History
persistently enlarged lymph nodes, constitutional or B symptoms (fever, rash, night sweats, and/or weight loss)
Exam
lymphadenopathy in one or more regions, hepatosplenomegaly may be present, fever, bulky mass in prevascular (anterior) mediastinum with signs consistent with superior vena cava syndrome indicates primary mediastinal B-cell lymphoma
1st investigation
- peripheral lymph node excision biopsy:
type and grade of non-Hodgkin lymphoma
More
Other investigations
- CBC:
anemia, pancytopenia
More - lactate dehydrogenase (LDH):
elevated; is a sign for disease activity and a prognostic marker
More - bone marrow biopsy:
lymphoma cells may be present in bone marrow
More - CT scan of neck, chest, abdomen, and pelvis:
evaluation of the extent of lymphadenopathy and staging
More - 18F-FDG PET-CT scan of neck, chest, abdomen, and pelvis:
evaluation of the extent of lymphadenopathy and staging
- HIV serology:
may be positive
More - hepatitis B and C serology:
may be positive
More
Metastatic cancer
History
prior cancer history in the presence of new lymphadenopathy should raise suspicion for recurrent or metastatic disease; patients may complain of fatigue, weight loss, and other constitutional symptoms
Exam
weight loss, occasionally fever, pallor; other physical exam findings vary according to the cancer type
1st investigation
- biopsy:
identification of malignant cells in lymph node
More
Other investigations
- CBC:
anemia may be present in any malignancy; pancytopenia may indicate bone marrow infiltration
- CT scan:
staging; identify primary tumor or other sites of metastasis; lymph nodes may have central necrosis
- PET scan:
staging; identify primary tumor or other sites of metastasis
- Gallium 68 PET scan:
staging; identify metastatic neuroendocrine tumor
Thymoma
History
presenting symptoms depend on tumor location, size, growth rate, and paraneoplastic syndromes; half of patients with thymomas are asymptomatic; in symptomatic patients, 40% have myasthenic symptoms; paraneoplastic syndromes include myasthenia gravis, limbic encephalitis, pure red cell aplasia; symptoms include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea related to tumor compression or invasion; myasthenic manifestations include easy fatigability, ptosis, diplopia, dysarthria; limbic encephalitis manifestation includes mood or behavioral changes, cognitive dysfunction
Exam
often asymptomatic; airway compression (stridor, prolonged inspiration/expiration); recurrent laryngeal nerve compression (hoarseness); superior vena cava obstruction (facial swelling, collateral veins, plethora); myasthenic manifestations (easy fatigability, ptosis, diplopia, dysarthria); limbic encephalitis (cognitive dysfunction, complex partial seizures, hyperthermia)
1st investigation
- CT scan of chest:
enlarged thymus often with well-defined borders and preservation of fat planes; local invasion may be present
More - MRI:
distinguishes between cysts, thymic neoplasm, and thymic hyperplasia
Other investigations
- acetylcholine receptor antibody:
elevated titer (range varies with assay used)
More - CBC:
anemia may be a result of paraneoplastic pure red cell aplasia
- biopsy:
only necessary when prevascular (anterior) mediastinal mass appears infiltrative or invasive, which often requires neoadjuvant therapy; if mass is characteristic of a resectable thymoma, preoperative biopsy is generally avoided
More
Lung cancer
History
may present with cough, dyspnea, hemoptysis, chest pain, weight loss; fatigue, hoarseness, dysphagia; bone metastases suspected if bone pain and/or fractures; brain metastases suspected if confusion, personality changes, nausea and vomiting, headache, seizures present
Exam
wheeze, rales, decreased breath sounds, and dullness to percussion; cervical or supraclavicular adenopathy, finger clubbing, hypertrophic osteoarthropathy; in superior vena cava (SVC) syndrome: facial swelling, dilated neck or chest/abdominal wall veins
1st investigation
- CXR:
non-small cell lung cancer (NSCLC): variable; may detect single or multiple pulmonary nodule(s), mass, pleural effusion, lung collapse, or mediastinal or hilar fullness; small cell lung cancer (SCLC): central or peripheral mass, hilar lymphadenopathy, superior mediastinal lymphadenopathy, pleural effusion
- CT chest:
NSCLC: shows size, location, and extent of primary tumor; evaluates for hilar and/or mediastinal lymphadenopathy and distant metastases; SCLC: massive lymphadenopathy and direct mediastinal invasion are common features of SCLC; determines extent of disease
Other investigations
- bronchoscopy:
endobronchial lesions
- biopsy:
malignant cells, high nuclear to cytoplasmic ratio, nuclear fragmentation often present
- 18F-FDG PET-CT:
NSCLC: evaluates location and extent of primary tumor; evaluates for hilar and/or mediastinal lymphadenopathy and distant metastases
More
Uncommon
Aortic dissection
History
sudden-onset chest pain usually described as ripping or tearing; pain is often maximal at onset and changes as the dissection evolves; pain radiating into the neck or jaw may indicate that the dissection involves the aortic arch and extends into the great vessels of the arch; pain that is felt in the intrascapular area may indicate that the dissection involves the descending aorta; aortic dissection can be painless in about 10% of patients and especially in patients with collagen vascular disorder
Exam
hypertension may result from a catecholamine surge or underlying essential hypertension; hypotension may be the result of excessive vagal tone, cardiac tamponade, or hypovolemia from rupture of the dissection; neurologic deficits occur in 20% of cases; most common neurologic findings are syncope and altered mental status; dyspnea may be caused by congestive heart failure or tracheal or bronchial compression; new diastolic murmur from aortic insufficiency; asymmetric pulses and blood pressure measurements
1st investigation
Hodgkin lymphoma
History
persistently enlarged lymph nodes, constitutional or B symptoms (fevers, night sweats, and/or weight loss)
Exam
lymphadenopathy in one or more regions, hepatosplenomegaly may be present, fever
1st investigation
- peripheral lymph node excisional biopsy:
type of Hodgkin lymphoma
More
Other investigations
- CBC:
anemia or pancytopenia may be present
More - lactate dehydrogenase (LDH):
elevated; is a sign for disease activity and a prognostic marker
- CT scan of neck, chest, abdomen, and pelvis:
evaluation of the extent of lymphadenopathy and staging
More - PET-CT scan of neck, chest, abdomen, and pelvis:
evaluation of the extent of lymphadenopathy and staging
- bone marrow biopsy:
lymphoma cells may be present in bone marrow
More
Mediastinal germ cell tumor: seminoma
History
presenting symptoms depend on tumor location, growth rate, and size; seminomas tend to grow slowly and metastasize later than nonseminomas, and may reach a larger size at presentation; symptoms include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea; occurs in people ages 20 to 40 years, with male predominance
Exam
often asymptomatic, airway compression may present with stridor and prolonged inspiration/expiration; recurrent laryngeal nerve compression may present with hoarseness; superior vena cava obstruction may present with facial swelling, collateral veins, plethora; testicle exam may reveal testicle mass
1st investigation
- CT scan of chest, abdomen, and pelvis:
bulky, locally invasive mass; irregular borders; pulmonary and intrathoracic metastases may be seen
More
Other investigations
- biopsy:
type and grade of seminoma
More - serum beta-HCG:
may be elevated
More - serum alpha-fetoprotein:
negative; if elevated, nonseminomatous components are present
- testicular ultrasound:
testicular neoplasm may appear as well-defined hypoechoic lesions or inhomogeneous lesions with calcifications, cystic areas, and indistinct margins
More
Mediastinal germ cell tumor: nonseminoma
History
patients often have symptoms at presentation; symptoms include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea; constitutional symptoms include fever, chills, and weight loss
Exam
signs of airway compression (stridor, prolonged inspiration/expiration); signs of recurrent laryngeal nerve compression (hoarseness); signs of superior vena cava obstruction (facial swelling, collateral veins, plethora); testicle examination may reveal testicle mass; gynecomastia
1st investigation
- CT scan of chest, abdomen, and pelvis:
large lobulated inhomogeneous mass with thin capsule, may contain areas of hemorrhage and necrosis; mediastinal fat invasion commonly seen; pulmonary and intrathoracic metastases may be seen
Other investigations
Thymic carcinoma
History
majority of patients are symptomatic at presentation; symptoms may include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea; symptoms from tumor metastases may be present, such as bone pain or lymphadenopathy; may have constitutional symptoms of fever, weight loss, or sweats; paraneoplastic symptoms uncommon
Exam
signs of airway compression (stridor, prolonged inspiration/expiration); sign of recurrent laryngeal nerve compression (hoarseness); signs of superior vena cava obstruction (facial swelling, collateral veins, plethora)
1st investigation
- CT scan of chest, abdomen, and pelvis:
invasive, poorly defined mediastinal mass with obliteration on mediastinal fat plane; vascular invasion, lymphadenopathy, and extrathymic metastases are common; may also contain calcification and necrosis
More
Other investigations
- biopsy:
depends on type and grade of thymoma
More - CBC:
anemia may be a result of paraneoplastic pure red cell aplasia
Primary tracheal tumors
History
tracheal obstruction results in dyspnea, cough, and stridor (may be misdiagnosed as asthma in children); acute respiratory distress may not be present until the trachea is almost completely occluded; hemoptysis may occur
Exam
tracheal obstruction results in respiratory distress, cough, wheezing, and stridor
1st investigation
- CT scan of chest with contrast enhancement:
tumors are often small, solid, and located within the tracheal lumen; extratracheal invasion may be present
More
Neurogenic tumor
History
no gender predilection; commonly occurs in young adults; asymptomatic in majority of adults but only 20% of children; children commonly present with respiratory symptoms such as dyspnea and cough; if associated with neurofibromatosis, multiple skin neuromas are present; depending on size and location, tumors may result in spinal cord compression, pain, numbness, weakness, and muscle atrophy
Exam
hypertension and/or tachycardia, may be a sign of a catecholamine-secreting tumor; classic triad of pheochromocytoma may present with headache, sweats, and tachycardia; airway compression may present with stridor, prolonged inspiration/expiration; recurrent laryngeal nerve compression may present with hoarseness; superior vena cava obstruction may present with facial swelling, collateral veins, plethora
1st investigation
- CT scan of chest with contrast enhancement:
almost always located in paravertebral (posterior) mediastinum along costovertebral sulcus; rounded or spindle- or dumbbell-shaped mass; spinal invasion or spinal canal extension; intratumoral calcification may be present
More
Other investigations
- metaiodobenzylguanidine (MIBG) scan:
defines extent and identifies other areas of involvement of a catecholamine-secreting tumor
More - plasma free metanephrines or 24-hour urine fractionated metanephrines and normetanephrines:
elevated levels support diagnosis of catecholamine-secreting tumor
More - biopsy:
results depend on type and grade of neurogenic tumor
More
Thyroid neoplasm
History
patients often have a known goiter; substernal extension may present with exertional dyspnea, positional dyspnea, stridor, wheezing, or cough
Exam
often painless solitary nodules; presence of goiter (80% to 90% of patients with substernal goiters have a visible goiter); hypertension and tachycardia may be a sign of thyrotoxicosis or pheochromocytoma; substernal extension suggested by inability to identify lower pole of thyroid gland; airway compression may present with stridor, prolonged inspiration/expiration; tracheal deviation if goiter is asymmetric; presence of Pemberton signs (neck vein distention and facial flushing when arms held vertically above head - Pemberton maneuver)
1st investigation
- CT scan of neck and chest without contrast enhancement:
determines extent and size of thyroid mass
More
Other investigations
- thyroid-stimulating hormone:
usually elevated if hypothyroid, normal if euthyroid, or suppressed if hyperthyroid
- thyroglobulin and anti-thyroglobulin antibody levels:
may be elevated in thyroid cancer but not in medullary thyroid cancer
More - calcitonin level:
may be elevated in medullary thyroid cancer
More - radioactive iodine thyroid scan:
"cold" nodule may be indicative of a thyroid neoplasm
More - MRI neck and chest:
assesses relationship of mass to vascular structures
More - biopsy:
result depends on type and grade of thyroid tumor
More
Substernal goiter
History
history of known goiter; exertional or positional dyspnea; stridor or wheezing; cough; hyperthyroidism symptoms (heat intolerance, weight loss, insomnia)
Exam
80% to 90% of patients with substernal goiters have a visible goiter; substernal extension suggested by inability to identify lower pole of thyroid gland; airway compression may present with stridor, prolonged inspiration/expiration; sign of thyrotoxicosis (weight loss, hypertension, and tachycardia); tracheal deviation if goiter is asymmetric, presence of Pemberton signs (neck vein distention and facial flushing when arms held vertically above head - Pemberton maneuver)
1st investigation
- CT scan of neck and chest without contrast enhancement:
determines extent and size of thyroid
More
Other investigations
- thyroid-stimulating hormone:
usually elevated if hypothyroid, normal if euthyroid, or suppressed if hyperthyroid
- MRI neck and chest:
assesses relationship of mass to vascular structures
More
Acute lymphocytic leukemia (ALL)
History
fatigue, dyspnea, dizziness, bleeding, easy bruising, and recurrent infections
Exam
pallor and ecchymoses, and rarely lymphadenopathy and hepatosplenomegaly
1st investigation
- CBC:
anemia, leukocytosis, leukopenia, and/or thrombocytopenia
Other investigations
- bone marrow biopsy:
bone marrow hypercellularity and infiltration by leukemic lymphoblasts
- molecular studies:
to detect genetic abnormalities associated with ALL
More - mediastinoscopy and biopsy:
performed if marrow or peripheral blood testing is nondiagnostic
Chronic lymphocytic leukemia
History
age >60 years; frequently asymptomatic and detected as an incidental finding on blood tests for another reason; B symptoms: fever, chills, night sweats, weight loss, and fatigue
Exam
painless peripheral lymphadenopathy, splenomegaly
1st investigation
- CBC:
elevated WBC count with absolute lymphocytosis >5000/microliter; anemia and thrombocytopenia may be present
- blood film:
smudge cells present
More
Other investigations
- flow cytometry on peripheral blood:
CD5, CD19, and CD23 positive
More - bone marrow biopsy:
>30% of the cells are lymphocytes
- mediastinoscopy and biopsy:
performed if marrow or peripheral blood testing is nondiagnostic or if there is suspicion that mediastinal lymphadenopathy is a different process
Pericardial cyst
History
thin-walled cysts that arise from the pericardium; almost always asymptomatic and identified incidentally; signs of congestive heart failure (dyspnea, edema, fatigue, and palpitations)
Exam
hemodynamic compromise may occur depending on size and location of lesion; signs of congestive heart failure (edema, elevated jugular venous pressure); arrhythmia (atrial fibrillation) may also be present
1st investigation
- CT scan of chest with contrast enhancement:
nonenhancing, thin-walled, well-defined, homogeneous masses; attenuation is close to water density
More
Other investigations
- MRI:
cysts have low signal intensity on T1 weighted images and high signal intensity on T2 weighted images
More
Bronchogenic cyst
History
occurs in both adults and children without gender predilection; may be asymptomatic and identified incidentally; chest pain and dysphagia are most common presenting symptoms; consider bronchogenic cyst in patients with recurrent lung infections
Exam
signs of airway compromise (cough, wheezing, dyspnea, and respiratory distress); signs of infection (fever, purulent sputum, cough)
1st investigation
- CXR:
well-defined round mass often located in the vicinity of the carina; air-fluid level may be present
More
Other investigations
- CT scan of chest with contrast enhancement:
nonenhancing, thin-walled, well-defined, homogeneous masses; cyst may contain blood, pus, or secretions; calcifications may be present
More
Esophageal cyst (includes esophageal duplication cyst)
History
almost always asymptomatic and identified incidentally; often present during childhood; chest tightness or fullness and dysphagia may be present
Exam
almost always asymptomatic
1st investigation
- CT scan of chest with contrast enhancement:
nonenhancing, well-defined, homogeneous masses
More
Other investigations
- barium swallow:
demonstrates the presence of communication between cyst and esophagus lumen
More - endoscopy and endoscopic ultrasound (EUS):
identifies an esophageal duplication cyst to be a protruding, submucosal mass that is covered by normal epithelium; EUS differentiates between an intramural or extramural mass and delineates the relation of the cyst to surrounding structures
More
Mediastinal germ cell tumor: mature teratoma
History
often asymptomatic and is an incidental finding; presenting symptoms depend on tumor location and size; symptoms include chest pressure, hoarseness, chest wall pain, dysphagia, and dyspnea; can occur in any age group but more common in children or young adults, with no gender predilection
Exam
often asymptomatic; airway compression (stridor, prolonged inspiration/expiration); recurrent laryngeal nerve compression (hoarseness); superior vena cava obstruction (facial swelling, collateral veins, plethora)
1st investigation
- CT scan of chest, abdomen, and pelvis:
mass may be solid or cystic; well delineated from surrounding tissue; fat-fluid level or fatty mass with globular calcification may be seen; tumor may have a calcified capsule and occasionally contain teeth
More
Use of this content is subject to our disclaimer