Tests
1st tests to order
CBC
Test
White cells are usually elevated with a polymorphonuclear predominance. However, can be normal, particularly in the initial stages.
Leukopenia or neutropenia is not uncommon in neonates and in severe sepsis.
Thrombocytopenia may also be present in neonates and in severe sepsis.
Anemia may be present, particularly in cases of subacute or chronic infections such as osteomyelitis or endocarditis.
Result
leukocytosis, anemia, thrombocytopenia, leukopenia, neutropenia
BUN
Test
Metabolic abnormalities including renal impairment can develop in sepsis.
Result
normal or elevated BUN and creatinine
serum electrolytes
Test
Metabolic abnormalities can develop in sepsis.
Result
normal or deranged
serum glucose
Test
Metabolic abnormalities, including hyperglycemia (in diabetic patients) and hypoglycemia (in neonates), can develop in sepsis.
Result
normal, decreased, or elevated
coagulation studies
Test
Disseminated intravascular coagulation can accompany severe sepsis.
Result
normal, or prolonged prothrombin time, elevated fibrin degradation products, decreased fibrinogen or antithrombin levels, thrombocytopenia, and positive D-dimer
LFTs
Test
Alanine aminotransferase and aspartate aminotransferase can be nonspecifically elevated in sepsis.
Result
normal or elevated
C-reactive protein (CRP)
Test
As with any bacterial infection, CRP is typically elevated.
Degree of elevation depends on the site of infection and host factors.
In severe disease, CRP is usually >100 mg/L.
Result
normal or elevated
blood culture
Test
Should be taken if infection is suspected, but giving antibiotics should not be delayed in meningitis or severe sepsis if blood cultures cannot be obtained immediately. [Figure caption and citation for the preceding image starts]: Group B streptococci on blood agarFrom the collection of Dr Brendan Healy [Citation ends].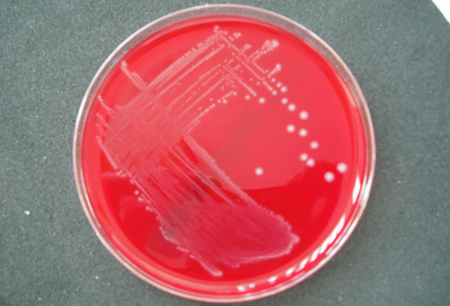
Definitive test for the diagnosis of sepsis.
Appropriate volumes of blood should be obtained according to the blood culture system used. Three sets of blood cultures should be taken from different sites at different times if endocarditis is suspected.
Antibiotics given before drawing of blood cultures significantly reduces the yield.
Negative blood cultures do not exclude infection.
Result
positive for GBS (sepsis)
cerebrospinal fluid (CSF) Gram stain
Test
CSF exam should be considered in patients with signs and symptoms of meningitis and in all neonates with sepsis.[64]
A positive Gram stain in the context of a compatible clinical situation may provide a rapid presumptive diagnosis of meningitis.
Gram stain indicates streptococcal infection but cannot reliably determine the type of streptococci.
Result
gram-positive cocci in chains (meningitis)
CSF culture
Test
CSF exam should be considered in patients with signs and symptoms of meningitis and in all neonates with sepsis.[64]
Confirms diagnosis of GBS meningitis.
Yield from CSF culture is reduced if antibiotics are given before obtaining CSF, and a negative culture does not therefore exclude the diagnosis.
Ideally, lumbar puncture should be carried out within 30 minutes of assessment.[71]
Result
positive for GBS (meningitis)
CSF cell count and differential
Test
CSF exam should be considered in patients with signs and symptoms of meningitis and in all neonates with sepsis.[64]
In bacterial meningitis, CSF cell counts typically range from 500 to 5000 cells/mm³ with a polymorphonuclear predominance of >60%.
In fulminant infections and in young infants, CSF cell counts may be only mildly elevated or normal.
In early bacterial meningitis, there may be a transient lymphocytic pleocytosis.[69]
Result
normal, polymorphonuclear pleocytosis, or transient lymphocytic pleocytosis (meningitis)
CSF glucose and protein
Test
CSF exam should be considered in patients with signs and symptoms of meningitis and in all neonates with sepsis.[64]
Most patients with bacterial meningitis have a CSF glucose concentration of ≤40 mg/dL or an absolute ratio of CSF to serum glucose concentrations ≤0.4.[69]
CSF protein is typically elevated.
In rapidly progressive infections, values may be only slightly abnormal or normal.
Result
normal or decreased glucose and elevated protein (meningitis)
antigen detection in CSF
Test
Antigen testing of the CSF can add weight to the diagnosis, but adds little to the patient management plan.
False-positive results do occur, and the tests should be used and interpreted with caution. Positive results are more reliable if they are matched by a compatible Gram film (e.g., gram-positive cocci in chains).
Result
positive latex agglutination test for GBS antigen (meningitis)
Gram stain and culture of other sterile body fluids
Test
Indicated if the clinical picture suggests a less common focus of infection (e.g., joint aspirate in septic arthritis, bone sample in osteomyelitis, urine in urinary tract infection, sputum in pneumonia, skin in cellulitis, aspirate of any collections of pus - e.g., in intra-abdominal infection and occasionally in sinusitis).[37][67] Urine culture should be performed for neonates with suspected late-onset disease.[64]
A positive Gram stain indicates streptococcal infection and can provide a rapid presumptive diagnosis. However, the exact type of streptococci cannot be reliably determined by the Gram film alone.
Positive culture confirms diagnosis.
Swabs for culture (but not Gram stain) should be sent in patients with conjunctivitis and otitis media if there is evidence of perforation of the ear drum.
Result
gram-positive cocci in chains on Gram stain; culture positive for GBS
chest x-ray
Test
Pneumonia can be confirmed on chest x-ray, but it does not provide information on causative organism.
Neonates with GBS infection typically have a diffuse pulmonary infiltrate.
Septic pulmonary emboli can occur in right-sided endocarditis.
Result
lobar consolidation, diffuse pulmonary infiltrates in neonates (pneumonia)
plain joint and/or bone x-ray
Test
Typical findings of septic arthritis and other bone and joint infections.[64]
Result
evidence of infection, examples include: joint-space widening or soft-tissue swelling (septic arthritis); osteopenia and evidence of bone destruction, cortical breaches, and periosteal reaction - may show joint effusion in local joints (osteomyelitis)
CT head
Test
Often done before lumbar puncture to exclude a contraindication to lumbar puncture such as elevated intracranial pressure, and is recommended in patients who are immunocompromised, have a history of central nervous system disease, have new-onset seizures, have papilledema, or have an abnormal level of consciousness or a focal neurologic deficit.[69]
May be useful if meningitis is diagnosed to assess for complications such as ventriculitis or brain abscess.[64]
Result
normal or elevated intracranial pressure or intracranial lesion if other pathologies present
Tests to consider
echocardiography
Test
Echocardiography should be carried out if endocarditis is suspected.
Transesophageal echo (TEE) has a higher sensitivity and specificity than transthoracic echo (TTE).
If a TTE is negative and the diagnosis is strongly suspected, a TEE should be carried out. In general, TTE provides poor images of the right side of the heart.
Result
valvular vegetation or abscess, valvular regurgitation (endocarditis)
MRI
Test
May be useful if meningitis is diagnosed to assess for complications such as ventriculitis or brain abscess.[64]
Result
normal or intracranial lesion if other pathologies present
Use of this content is subject to our disclaimer