Tests
1st tests to order
thrombophilia screening
Test
Acquired deficiencies of coagulation factors and inhibitors of coagulation can develop in the event of liver failure whether acute or chronic. Therefore, decreased levels of coagulation inhibitors are of significance only when associated with normal or slightly reduced levels of coagulation factors. Otherwise, the effect of liver insufficiency must be corrected using, for example, the factor II or X plasma levels.[33]
Result
positive gene mutation: factor V Leiden, G20210A prothrombin (factor II), or methylenetetrahydrofolate reductase; reduced serum level of protein C, protein S, or antithrombin III; elevated serum homocysteine level; positive lupus anticoagulant, anticardiolipin, and anti beta2 glycoprotein-1 antibodies (antiphospholipid syndrome)
color and pulsed Doppler ultrasound
Test
Sensitivity and specificity of >85%.[33]
Specific signs include alterations in hepatic and/or caval veins in the form of thrombosis, stenosis, fibrotic cord, or insufficient recanalization of the vessels.
Suggestive sonographic findings include intrahepatic venovenous, portovenous, or portacaval collaterals and caudate vein diameter >3 mm.
Nonspecific findings include caudate lobe hypertrophy, inhomogeneous liver parenchyma, extrahepatic collaterals, portal vein thrombosis, and regenerative nodules as well as ascites.
The combination of specific signs and caudate lobe hypertrophy has the highest predictive value to identify patients with Budd-Chiari syndrome.
Result
alterations in hepatic and/or caval veins in the form of thrombosis, stenosis, fibrotic cord, or insufficient recanalization of the vessels
LFTs
Test
Nonspecific but almost always elevated to some extent.
Significant elevation in serum aspartate and alanine aminotransferase levels to ≥5 times above the upper limit is usually seen in fulminant and acute forms of Budd-Chiari syndrome.
Levels of alkaline phosphatase and bilirubin may also increase along with a decrease in serum albumin.
Result
elevated aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, bilirubin; decreased albumin
BUN and creatinine
Test
Should be performed at baseline for all patients.
Result
elevated in fulminant BCS
coagulation profile
Test
Should also be performed at baseline before starting anticoagulant therapy.
Result
prolonged prothrombin time in fulminant BCS
CBC
Test
Evaluation of the peripheral blood may show evidence of a primary myeloproliferative disorder (MPD) such as polycythemia vera, essential thrombocytosis, or myelofibrosis. If the results are abnormal, other blood tests may be ordered.
Result
abnormal if underlying MPD
Janus kinase 2 (JAK2) mutation
Test
About 80% of patients with Budd-Chiari syndrome (BCS) with an myeloproliferative disorder (MPD) harbor JAK2(V617F) mutation; thus, JAK2 mutation testing has facilitated the diagnosis of an occult type of MPD.[3][39] One meta-analysis showed the pooled prevalence of JAK2(V617F) mutation was 37% in patients with BCS. After pre-existing MPD was excluded, the pooled prevalence was decreased to 26%.[40]
Testing for JAK2 mutation is done when the diagnosis of an MPD proves to be difficult, for example, if the typical changes in peripheral blood, such as high levels of hemoglobin, platelets, or white blood cells, are absent; or if conventional diagnostic criteria are not met
Result
positive if underlying MPD
flow cytometry for CD55- and CD59-deficient blood cells
Test
Fluoresceinated monoclonal antibodies to glycosylphosphatidylinositol-anchored proteins are used to detect the defective cells characteristic of paroxysmal nocturnal hemoglobinuria.[45]
Result
presence of deficient cells suggests paroxysmal nocturnal hemoglobinuria
Tests to consider
serum-ascites albumin gradient (SAAG)
Test
Nonspecific.
A high SAAG in combination with a total ascitic protein >2.5 g/dL supports a diagnosis of noncirrhotic Budd-Chiari syndrome (BCS), although the ascitic protein may be low in chronic BCS with concomitant cirrhosis. However, high SAAG with high protein ascites may also be seen in cardiac causes of ascites.
Result
high >1.1 (indicating portal hypertension as cause of ascites)
total ascitic protein
Test
Nonspecific.
A high serum-ascites albumin gradient (SAAG) in combination with a total ascitic protein >2.5 g/dL supports a diagnosis of noncirrhotic Budd-Chiari syndrome (BCS), although the ascitic protein may be low in chronic BCS with concomitant cirrhosis. However, high SAAG with high protein ascites may also be seen in cardiac causes of ascites.
Result
>2.5 g/dL
CT abdomen
Test
Used to visualize the hepatic veins and demonstrate occlusion of hepatic veins, inferior vena cava (IVC), or both. It also offers better visualization of liver parenchymal abnormalities and necrotic areas compared with sonography.[34]
It can also detect other lesions such as tumors, abscess, and cysts in secondary Budd-Chiari syndrome.
Result
occlusion of hepatic veins and/or IVC; areas with necrotic liver parenchyma; detect other lesions
MRI abdomen
Test
MRI is more accurate than CT and allows optimal delineation of venous obstruction for therapeutic decisions.[35]
It also differentiates acute form of Budd-Chiari syndrome from subacute and chronic disease and helps to exclude alternative diagnoses.
Result
thrombus, compression and/or stenosis along the whole length of the inferior vena cava or hepatic veins; necrosis and focal nodular hyperplasia in liver parenchyma; detect other lesions
hepatic venography
Test
Considered the definitive diagnostic tool in the diagnosis of Budd-Chiari syndrome (BCS). Hepatic venography is carried out when the suspicion of BCS is high, even in the absence of typical findings on other radiologic imaging. It should also be performed when percutaneous or surgical shunting is considered to measure the portacaval venous pressure gradient. [Figure caption and citation for the preceding image starts]: Hepatic venogram demonstrating "spider web" and thrombus in the inferior vena cavaLiver Transplantation Journal. 2006;12:S21-S22. Reprinted with permission of John Wiley & Sons, Inc [Citation ends].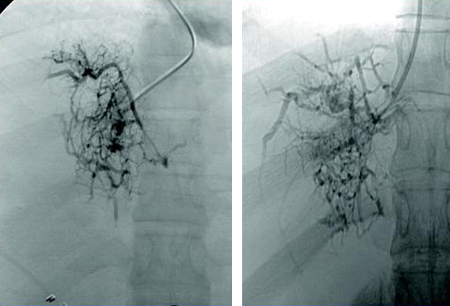
Result
spider web pattern
contrast-enhanced 3-dimensional magnetic resonance angiography
Test
Indicated when it is impossible to cannulate the hepatic veins during hepatic venography, and in patients with renal insufficiency, as venography usually requires the use of considerable amounts of iodine-containing contrast medium.
Provides the demonstration of vascular structures both in the liver and in the upper abdomen in various planes, and also yields information concerning the parenchymal status. It is also useful in evaluating treatment options and in assessing therapeutic effects in follow-up period.[37]
Result
visualization of thrombosis, compression or stenosis of hepatic veins and/or inferior vena cava; visualization of intrahepatic, extrahepatic collaterals, parenchymal necrosis, focal nodular hyperplasia
transjugular liver biopsy
Test
Liver biopsy is not required to confirm the diagnosis as the disease is heterogeneous, giving rise to high risk of sampling error.[43] Liver biopsy is not recommended as standard in children, adolescents, or young adults.[44] It is needed only in the small subset of patients in whom BCS is related to pure thrombotic involvement of the small hepatic veins, where major hepatic veins and inferior vena cava appear patent at imaging.[1]
Liver biopsy should be carried out at the same time as angiographic investigation, to assess liver reserve and potential reversibility of liver injury before shunting procedures.[46]
Result
centrilobular congestion, hepatocyte necrosis, fibrosis, and ultimately cirrhosis
bone marrow biopsy
Test
Required in cases of suspected myeloproliferative disorder (MPD) with negative JAK2 mutation.
Result
clusters of dystrophic megakaryocytes confirms MPD
Use of this content is subject to our disclaimer