Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
endoscopic thoracoscopic sympathectomy (ETS)
If symptoms persist, ETS may be considered.[31] The procedure is generally done on both sides at one sitting, under general anesthesia, and is a short-stay procedure in the majority of instances.
The specific hyperhidrosis disorder determines the level of the sympathetic procedure.
For example, surgery at the third (T3), fourth (T4), or fifth (T5) thoracic ganglia is for axillary hyperhidrosis.
Some controversy exists whether compensatory sweating is more problematic at higher sympathectomy levels, but patient selection is likely far more important.[32]
Sympathetic surgery at T3 or T4 can be expected to benefit 80% to 90% of patients with axillary hyperhidrosis. However, several studies have shown that sympathetic surgery in patients with axillary hyperhidrosis is less successful and that the level of patient satisfaction is lower than it is for patients with palmar hyperhidrosis.[14][33][34][35][36][37][38][40][Figure caption and citation for the preceding image starts]: Thoracoscopic view of the left upper posterior mediastinum with the sympathetic chain visualized over the 2nd, 3rd, and 4th costal heads (R2, R3, and R4, respectively)From the personal collection of Fritz Baumgartner, MD [Citation ends].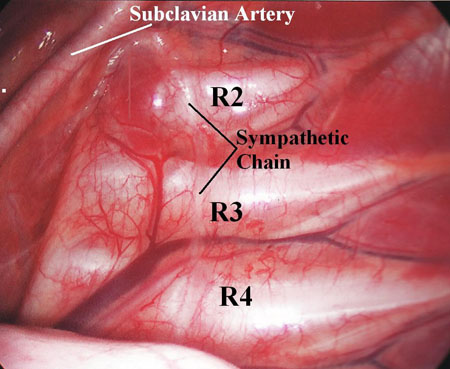
endoscopic thoracoscopic sympathectomy (ETS)
ETS is appropriate for severe, debilitating palmar sweating when other treatments have failed.[31]
In these cases, the expected benefits generally outweigh the known side effects, which may include compensatory sweating.[9][14]
The specific hyperhidrosis disorder determines the level of the sympathetic procedure. For example, surgery at the second (T2) or third (T3) thoracic ganglia is recommended for palmar hyperhidrosis.
ETS is also appropriate for patients with severe palmar and severe plantar hyperhidrosis (palmoplantar hyperhidrosis) when other treatments have failed. It is emphasized that the ETS procedure is meant to cure the palmar hyperhidrosis, and any benefit for the feet is never the primary intent of the surgery.
Surgery can be performed at the T2 or T3 level, although some suggest the T4 level. The best level to select is unclear and controversial. Surgery at the T2 level may be more consistently curative with less dramatic failures than at T3,[49][50] but is associated with an increased incidence of compensatory hyperhidrosis postoperatively.[48][49][50] However, excellent long-term results with a low (1.3%) rate of severe compensatory sweating have been reported by some using the T2 level.[52]
Successful outcomes for palmar sweating are achieved in >95% of cases.[51] Plantar sweating is improved in the short term in approximately 80% of cases, although not as dramatically as the palmar sweating.
Because of the higher incidence of moderate or severe compensatory hyperhidrosis, some recommend avoiding T2 procedures altogether, although others report excellent results using the T2 level.[49][52] Some even recommend levels of sympathetic intervention for palmoplantar hyperhidrosis at levels lower than T3 (i.e., over the 4th or 5th rib levels), although this may result in "moister hands".[48] It is suggested that proper patient selection is far more important than sympathectomy level in achieving patient satisfaction regarding compensatory sweating.[15] Some surgeons perform ramicotomy rather than sympathetic nerve/ganglion intervention to limit the severity of compensatory sweating. However, the incidence of recurrent sweating does seem to be higher with ramicotomy.[53] Thoracoscopic sympathetic intervention can be safe and effective in younger patients, even in early teenage years, and has been shown to result in markedly improved long-term quality of life compared to nonoperative cohorts.[54][Figure caption and citation for the preceding image starts]: Thoracoscopic view of the right upper posterior mediastinum with the sympathetic chain visualized over the 2nd and 3rd rib costal heads (R2 and R3, respectively). Transection of the sympathetic chain at the level of T2 on the right and left sides is curative for palmar hyperhidrosisFrom the personal collection of Fritz Baumgartner, MD [Citation ends].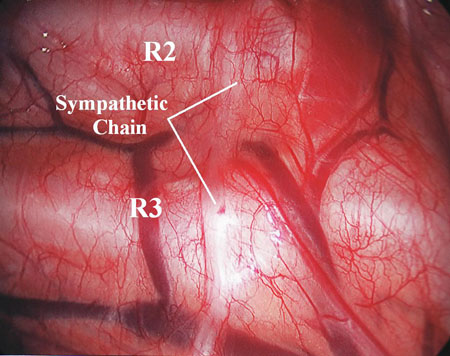 [Figure caption and citation for the preceding image starts]: Thoracoscopic view of the left upper posterior mediastinum with the sympathetic chain visualized over the 2nd, 3rd, and 4th costal heads (R2, R3, and R4, respectively)From the personal collection of Fritz Baumgartner, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Thoracoscopic view of the left upper posterior mediastinum with the sympathetic chain visualized over the 2nd, 3rd, and 4th costal heads (R2, R3, and R4, respectively)From the personal collection of Fritz Baumgartner, MD [Citation ends].
endoscopic thoracoscopic sympathectomy (ETS)
ETS is used for craniofacial sweating, although there is a higher incidence of patient dissatisfaction and complaints of compensatory sweating compared with palmar hyperhidrosis.[14][33][34][35][36][37][38][39][40] Treatment of craniofacial hyperhidrosis surgically should be considered very carefully as the side effects can be severe.
However, most patients with craniofacial hyperhidrosis will have significant benefit from sympathetic surgery at the T2 level. [Figure caption and citation for the preceding image starts]: Thoracoscopic view of the right upper posterior mediastinum with the sympathetic chain visualized over the 2nd and 3rd rib costal heads (R2 and R3, respectively). Transection of the sympathetic chain at the level of T2 on the right and left sides is curative for palmar hyperhidrosisFrom the personal collection of Fritz Baumgartner, MD [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer