Meniscal tear
- Overview
- Theory
- Diagnosis
- Management
- Follow up
- Resources
Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
all patients
rest, ice, compression, and elevation
Initially all patients should be treated with rest, ice, compression of the knee with an elastic bandage, and elevation of the leg above the level of the heart (RICE). This protocol helps to reduce pain, minimize swelling, and protect the injured tissue, all of which help speed up the healing process.
The use of crutches or a knee brace may be helpful with painful displaced bucket handle tears.
physical therapy
Treatment recommended for ALL patients in selected patient group
Programs designed to improve knee joint range of motion, core and leg strength, and knee stability, and to normalize gait are recommended.
Physical therapy is not necessary for small meniscal tears to heal but is beneficial for addressing gait abnormalities and strengthening the leg muscles that surround and stabilize the knee joint.
analgesia
Treatment recommended for SOME patients in selected patient group
Acetaminophen is the preferred drug for reducing pain because it acts centrally and does not interfere with the healing process.[34]Bergenstock M, Min W, Simon AM, et al. A comparison between the effects of acetaminophen and celecoxib on bone fracture healing in rats. J Orthop Trauma. 2005 Nov-Dec;19(10):717-23. http://www.ncbi.nlm.nih.gov/pubmed/16314720?tool=bestpractice.com
Nonsteroidal anti-inflammatory drugs (NSAIDs) should be used only for short periods because of the negative effects on musculoskeletal healing.[33]O'Connor JP, Lysz T. Celecoxib, NSAIDs and the skeleton. Drugs Today (Barc). 2008 Sep;44(9):693-709. http://www.ncbi.nlm.nih.gov/pubmed/19137124?tool=bestpractice.com
Primary options
acetaminophen: 325-1000 mg orally every 4-6 hours when required, maximum 4000 mg/day
Secondary options
ibuprofen: 400-800 mg orally every 4-6 hours when required, maximum 2400 mg/day
OR
meloxicam: 7.5 mg orally once or twice daily when required, maximum 15 mg/day
OR
naproxen: 500 mg orally initially, followed by 250 mg every 6-8 hours when required, maximum 1250 mg/day
surgery
Treatment recommended for SOME patients in selected patient group
Arthroscopic surgery should be considered for those with large (≥1 cm) meniscal tears, root tears, and cases where symptoms persist despite nonoperative care to prevent further damage and save healthy meniscus tissue. Suturing of the tissue is possible if a stable repair can be achieved (usually reserved for clear, clean pattern tears). [Figure caption and citation for the preceding image starts]: Arthroscopic view of horizontal cleavage tear of lateral meniscus (arrow)From the collection of Dr Kevin R. Stone [Citation ends].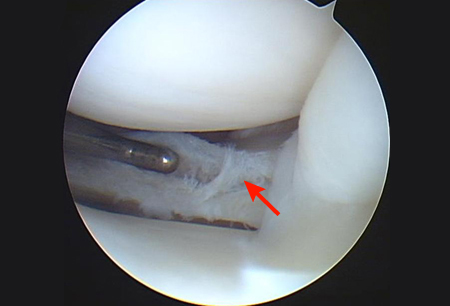 [Figure caption and citation for the preceding image starts]: Arthroscopic view of suture repair of lateral meniscus (arrow)From the collection of Dr Kevin R. Stone [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic view of suture repair of lateral meniscus (arrow)From the collection of Dr Kevin R. Stone [Citation ends]. Meniscal repair should only be used to heal peripheral meniscal lesions affecting healthy meniscal tissue in vascularized areas.[38]Beaufils P, Becker R, Kopf S, et al. The knee meniscus: management of traumatic tears and degenerative lesions. EFORT Open Rev. 2017 May;2(5):195-203.
https://www.doi.org/10.1302/2058-5241.2.160056
http://www.ncbi.nlm.nih.gov/pubmed/28698804?tool=bestpractice.com
More than 80% of meniscal tears in the central third (red-white zone) can heal by surgery.[39]Barber-Westin SD, Noyes FR. Clinical healing rates of meniscus repairs of tears in the central-third (red-white) zone. Arthroscopy. 2014 Jan;30(1):134-46.
http://www.arthroscopyjournal.org/article/S0749-8063(13)01120-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/24384277?tool=bestpractice.com
See Popliteal cyst for more information.
Meniscal repair should only be used to heal peripheral meniscal lesions affecting healthy meniscal tissue in vascularized areas.[38]Beaufils P, Becker R, Kopf S, et al. The knee meniscus: management of traumatic tears and degenerative lesions. EFORT Open Rev. 2017 May;2(5):195-203.
https://www.doi.org/10.1302/2058-5241.2.160056
http://www.ncbi.nlm.nih.gov/pubmed/28698804?tool=bestpractice.com
More than 80% of meniscal tears in the central third (red-white zone) can heal by surgery.[39]Barber-Westin SD, Noyes FR. Clinical healing rates of meniscus repairs of tears in the central-third (red-white) zone. Arthroscopy. 2014 Jan;30(1):134-46.
http://www.arthroscopyjournal.org/article/S0749-8063(13)01120-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/24384277?tool=bestpractice.com
See Popliteal cyst for more information.
Partial meniscectomy for complex pattern tear should be limited as far as possible, and necessitates careful patient selection; there may be no difference in outcomes between those undergoing partial meniscectomy for traumatic tear or those for degenerative tear (for whom arthroscopy is no longer recommended).[1]Kopf S, Beaufils P, Hirschmann MT, et al. Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1177-94. https://link.springer.com/article/10.1007/s00167-020-05847-3 http://www.ncbi.nlm.nih.gov/pubmed/32052121?tool=bestpractice.com [40]Abram SGF, Judge A, Beard DJ, et al. Adverse outcomes after arthroscopic partial meniscectomy: a study of 700 000 procedures in the national Hospital Episode Statistics database for England. Lancet. 2018 Nov 17;392(10160):2194-202. https://www.doi.org/10.1016/S0140-6736(18)31771-9 http://www.ncbi.nlm.nih.gov/pubmed/30262336?tool=bestpractice.com [41]Thorlund JB, Englund M, Christensen R, et al. Patient reported outcomes in patients undergoing arthroscopic partial meniscectomy for traumatic or degenerative meniscal tears: comparative prospective cohort study. BMJ. 2017 Feb 2;356:j356. https://www.doi.org/10.1136/bmj.j356 http://www.ncbi.nlm.nih.gov/pubmed/28153861?tool=bestpractice.com [42]Eijgenraam SM, Reijman M, Bierma-Zeinstra SMA, et al. Can we predict the clinical outcome of arthroscopic partial meniscectomy? A systematic review. Br J Sports Med. 2018 Apr;52(8):514-21. https://www.doi.org/10.1136/bjsports-2017-097836 http://www.ncbi.nlm.nih.gov/pubmed/29183885?tool=bestpractice.com
A complete meniscectomy, involving removal of the entire meniscus, is rarely performed and usually reserved for cases where the tear is large or cuts through the entire meniscus.
Associated ligamentous injury of the knee leads to knee instability. Therefore, in meniscal tears associated with such injuries, concomitant repair of the affected ligament should be considered, as meniscal repairs should be carried out on a stable knee.
postoperative measures
Treatment recommended for ALL patients in selected patient group
Postoperative care of the repaired or resected meniscus focuses on limiting axial load and rotational movement for the first month, followed by range-of-motion and strengthening exercises.
Partial meniscectomy: icing and elevation of knee above the level of the heart, use of crutches for first week, and progression to weight bearing as tolerated. Intra-articular hyaluronate injection may decrease postoperative pain and swelling.[44]Waddell DD, Bert JM. The use of hyaluronan after arthroscopic surgery of the knee. Arthroscopy. 2010 Jan;26(1):105-11. http://www.ncbi.nlm.nih.gov/pubmed/20117634?tool=bestpractice.com
Meniscal repair: similar to above; however, full weight bearing should be delayed for at least 4-6 weeks and range of movement of the knee, especially full flexion, should be limited to reduce strain on the repair site. Should not return to pivoting or knee-twisting sports (e.g., American football, soccer, rugby, basketball) for 2 months after meniscal repair.[12]Snoeker BA, Bakker EW, Kegel CA, et al. Risk factors for meniscal tears: a systematic review including meta-analysis. J Orthop Sports Phys Ther. 2013 Jun;43(6):352-67. https://www.jospt.org/doi/10.2519/jospt.2013.4295?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed http://www.ncbi.nlm.nih.gov/pubmed/23628788?tool=bestpractice.com
A knee brace is not usually indicated following meniscectomy. After meniscal repair the need for a brace depends on patient activity and condition of repair.
Primary options
sodium hyaluronate: consult specialist for guidance on dose
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer