Case history
Case history #1
A 45-year-old CMV-seronegative (CMV R-) man presents with 1 week of fever, malaise, and diarrhea. Five months prior to this clinical illness, he received a kidney transplant from a CMV-seropositive (CMV D+) donor. He has a history of long-standing diabetes mellitus that was complicated by end-stage renal failure. He received valganciclovir prophylaxis for the first 6 months after kidney transplantation. Laboratory examination shows leukopenia, thrombocytopenia, and elevated serum levels of creatinine, alanine aminotransferase (ALT), and aspartate aminotransferase (AST). Colonoscopic examination shows severe hyperemia and mucosal ulcerations involving the entire length of the colon.
Case history #2
A 35-year-old man with uncontrolled HIV infection and AIDS complains of a 2-week history of visual floaters and blurring of vision involving both eyes. His HIV RNA load is >750,000 copies/mL and his CD4 cell count is 2 cells/microliter. Physical examination reveals a severely cachectic man with enlarged cervical, axillary, and inguinal lymph nodes. Ophthalmologic examination reveals creamy-colored areas with overlying retinal hemorrhages, consistent with a diagnosis of chorioretinitis.[Figure caption and citation for the preceding image starts]: Fundoscopy (left eye) showing area of CMV retinitis inferonasally involving the vascular arcades and the optic disk, associated with vasculitis, and flame hemorrhagesAdapted from BMJ Case Reports 2009, copyright © 2009 by the BMJ Publishing Group Ltd [Citation ends].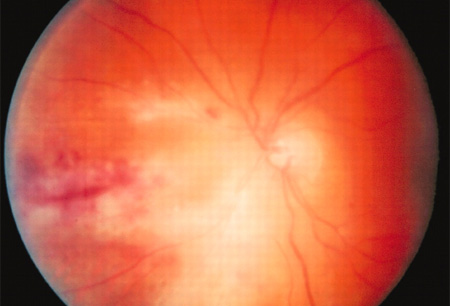
Other presentations
In immunocompetent patients with no significant medical history, cytomegalovirus (CMV) infection may present as a mononucleosis-like syndrome with fever, body aches, and malaise. Enlarged cervical lymph nodes may be present. Laboratory examination may reveal atypical lymphocytosis, normal renal function, and mildly elevated hepatic aminotransferases. Clinical symptoms usually resolve within 1 week, although severe end-organ disease has been described in some immunocompetent patients.
In patients with inflammatory bowel disease refractory to conventional treatment, CMV is implicated as a cofactor because the virus has been demonstrated in colon biopsies. Some patients have responded to treatment with intravenous ganciclovir.[5]
In critically ill people who require admission to the intensive care unit, such as those with sepsis, asymptomatic CMV reactivation may occur and may be associated with higher all-cause mortality.[6]
Congenital CMV infection in newborns can result in microcephaly, intracranial calcification, hepatosplenomegaly, neurologic abnormalities (presenting as poor tone and motor function), petechiae or purpura, and hearing loss.[7][8][9] Intellectual disability and sensorineural deafness are long-term complications.[10]
Use of this content is subject to our disclaimer