History and exam
Key diagnostic factors
common
subjective decrease in vision
Cataracts classically present as a gradual decrease in vision over many years that the patient may be very slow to recognize until there is some visual impairment.
However, under certain circumstances (e.g., diabetes mellitus), there may be a relatively sudden reduction in vision.[22]
blurred or cloudy vision
Changes in the lens lead to a decrease in its transparency, increased light scatter, and reduced vision.
glare
Frequently described, especially when driving at night.
washed-out color vision
In nuclear cataracts, the change in lens proteins often causes a yellowish hue to the cataract. Patients notice a decreased richness in colors, especially blues.
reduced visual acuity
Patients with a significant cataract exhibit a reduced best-corrected visual acuity.
Visual acuity should be tested with the patient's best-corrected spectacle correction at standardized distance and illumination conditions for both near and far vision.
blunted red reflex
May be seen during direct ophthalmoscopy.
Other diagnostic factors
common
inadequate glasses prescription
A patient with a progressing nuclear sclerotic cataract may also complain of inadequate glasses prescription.
The thickening of the lens can cause an increase in refractive power and make the patient appear increasingly myopic.
disruption of activities of daily living
Vision changes may affect activities of daily living, such as reading or driving.
Risk factors
strong
age >60 years
The prevalence of cataract increases with age, especially after age 60 years.[3]
Changes in lens proteins increase with age and reduce transparency. Increased age allows more time for formation of cortical (outer) layers of the lens, which reduces the ability of the lens to accommodate.
female sex
smoking
Smoking has been reported to be a risk factor for cataract.[18][19][20][21]
Oxidative stress has been linked to changes in crystalline lens proteins leading to the formation of cataract.
Moderate nuclear cataracts have been found to occur more frequently in nonwhite women who are smokers, and have large macular drusen (retinal metabolic byproducts that are normally removed).[1]
long-term UV exposure
Experimental evidence shows that the lens is susceptible to ultraviolet (UV) damage.
Changes in lens proteins, caused by aging or mutation, can lead to beta-crystallin protein aggregation when exposed to UV radiation.[2]
diabetes mellitus
eye trauma
Cataracts may be associated with blunt or penetrating injury to the globe.[Figure caption and citation for the preceding image starts]: Traumatic cataract and iris traumaFrom the personal collection of M. Bowes Hamill, MD [Citation ends].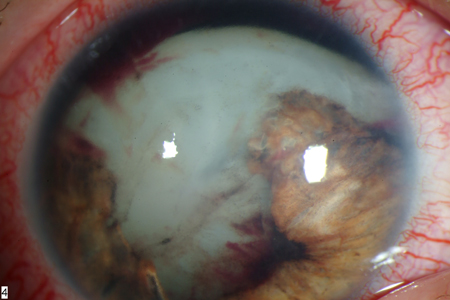
long-term corticosteroid use
family history of congenital cataract or congenital influences (e.g., toxins)
Lamellar or zonular cataracts are the most commonly seen form of congenital cataracts. These are usually bilateral and symmetric.
Cataracts may be due to transient toxic influences during lens development, or may be inherited in an autosomal-dominant pattern.
uveitis
myopia
The development of nuclear and posterior subcapsular cataract is associated with myopia.[25]
weak
other metabolic or hereditary conditions
Conditions (including galactosemia, Wilson disease, Marfan syndrome, and myotonic dystrophy) may be associated with particular types of cataract (e.g., Christmas tree cataract in people with myotonic dystrophy; sunflower cataract in people with Wilson disease).
Strength of association varies depending on each condition.
exposure to ionizing radiation
Healthcare workers who are exposed to ionizing radiation through medical imaging may be at increased risk of cataracts, particularly those involved in interventional cardiology procedures.[26]
Use of this content is subject to our disclaimer