Etiology
Hearing loss is one of the most common sensory impairments and can occur in patients of all ages. It can:
occur as an isolated symptom or as part of a symptom complex
gradual, progressive, or sudden
temporary or permanent.
External ear
Mechanical obstructions
Anything that blocks the transmission of sound through the ear canal to the tympanic membrane through to the ossicular chain can cause a conductive hearing loss. Many of these lesions can be identified on physical exam.
Impacted ear wax (cerumen) is one of the most common causes of hearing impairment and is present in 1 in 10 children, 1 in 20 adults, and one third of older and developmentally delayed patients.[4][5][6][7] Cerumen is a natural substance secreted by the glands of the external ear and also contains exfoliated skin cells from the ear canal. Cerumen serves many important functions, including canal lubrication and debris clearance, and it also has antibacterial properties. Cerumen impaction is one of the most common ear complaints and reasons for visiting a physician.[7][8] In addition to hearing loss, cerumen impaction can cause pain, itching, tinnitus, odor, drainage, dizziness, and cough.[4] Hearing loss due to cerumen can vary from 5 to 40 decibels (dB) depending on the degree of impaction.[5][8] It requires a narrowing of the ear canal of approximately 80% to cause hearing loss.[9] There are various methods to clean the ear canal, including irrigation, manual removal, and cerumenolytics.[7] Water and saline may be as effective as other cerumenolytics.[10]
Foreign bodies can lodge in the ear when placed there by children or, in adolescents and adults, when scratching the ear canal or trying to remove cerumen. They cause discomfort and, rarely, severe ear-canal infections. Fatal otogenic mastoiditis with a brain abscess from a retained cotton-applicator tip has been reported.[11] Insects may enter the ear canal while people are outdoors or while sleeping. They become lodged because they cannot turn around in the narrow space of the canal. [Figure caption and citation for the preceding image starts]: Foreign body in ear canalFrom the collection of Dr Richard Buckingham [Citation ends].
 [Figure caption and citation for the preceding image starts]: Insect in ear canal with pressure equalization tube visible anteriorlyFrom the collection of Dr Richard Buckingham [Citation ends].
[Figure caption and citation for the preceding image starts]: Insect in ear canal with pressure equalization tube visible anteriorlyFrom the collection of Dr Richard Buckingham [Citation ends].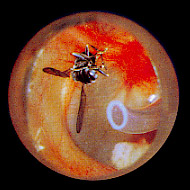
Cancers of the ear are rare and usually present with a painful, bleeding ear-canal mass and potential hearing loss due to obstruction of the ear canal. The most common type of cancer is squamous cell carcinoma and it usually arises in a patient with a history of chronic suppurative otitis media.[12] Any persistent granulation tissue in an ear canal may indicate cancer.[Figure caption and citation for the preceding image starts]: Squamous cell carcinoma of the ear canalFrom the collection of Dr Richard Buckingham [Citation ends].
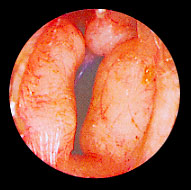
Exostoses are hard bony asymptomatic masses of the ear canal. They are usually multiple, bilateral, and broad-based, and are typically associated with a history of swimming in cold water.[13] Osteomas, by contrast, are usually solitary, are present only in 1 ear, have a narrow stalk, and are less common than exostoses.[14] Benign polyps are rare but may also cause obstruction and hearing loss.[Figure caption and citation for the preceding image starts]: Ear canal with bony narrowing secondary to exostosesFrom the collection of Dr Richard Buckingham [Citation ends].
Trauma
Minor ear-canal trauma includes excoriations, lacerations, and hematoma. Most ear-canal trauma occurs when patients attempt to clean or instrument the ear canal. Patients taking blood-thinning agents, such as warfarin, can bleed from minor trauma, and this bleeding can block the canal, causing hearing loss.
Congenital
Congenital malformations include atresia or stenosis of the ear canal. This may be an isolated finding or found in association with other abnormalities as part of a syndrome, such as Crouzon, Pierre Robin, or Apert syndromes. Crouzon is a genetic syndrome inherited in an autosomal-dominant manner, which results in premature fusion of some of the skull bones. This results in a myriad of features including low-set ears, hypertelorism, and exophthalmos (due to shallow eye sockets from early bony fusion). Pierre Robin syndrome is not due to a single gene defect but a defect in development and is characterized by micrognathia. Apert syndrome is a branchial arch disorder resulting in developmental abnormalities of the facial and skull bones, hands, and feet.
Local infections
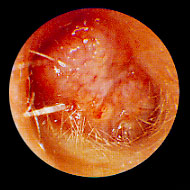
External ear infections are common and typically present with ear pain and ear drainage, but with further edema and inflammation of the canal, hearing loss can develop.[15] More than 90% of cases are caused by bacteria, most commonly Pseudomonas aeruginosa or Staphylococcus aureus.[16] Fungal infection is uncommon and may occur following treatment with topical antibiotics.[15] [Figure caption and citation for the preceding image starts]: Swollen ear canal, almost completely closed due to acute otitis externaFrom the collection of Dr Richard Buckingham [Citation ends].
 [Figure caption and citation for the preceding image starts]: Otomycosis: fungal debris in ear canalFrom the collection of Dr Richard Buckingham [Citation ends].
[Figure caption and citation for the preceding image starts]: Otomycosis: fungal debris in ear canalFrom the collection of Dr Richard Buckingham [Citation ends].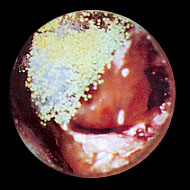
In patients with diabetes or in immunocompromised patients, the infection can spread into the deep tissues of the ear canal, resulting in necrotizing otitis externa, which can be fatal.[17][18][19] Irrigation of the ear canal with tap water has been reported to be a risk factor for necrotizing otitis externa in patients with diabetes.[20][21] This may be secondary to the characteristics of their cerumen, which is less acidic than in patients without diabetes.[22]
Middle ear
Local infections (current or recent)
A red, bulging, painful tympanic membrane indicates acute otitis media, a common presenting complaint in children.[23] The infection can be bacterial or viral; fever, ear pain, and discharge from the ear may be present. Acute otitis media has a high incidence (70%) of spontaneous improvement, so treatment is focused on symptomatic relief and prevention of sequelae, such as tympanic membrane perforation or chronic infection and subsequent effusion.[24][25][Figure caption and citation for the preceding image starts]: Erythematous bulging tympanic membrane due to acute otitis mediaFrom the collection of Dr Richard Buckingham [Citation ends].
 [Figure caption and citation for the preceding image starts]: Right tympanic membrane perforationFrom the collection of Dr Richard Buckingham [Citation ends].
[Figure caption and citation for the preceding image starts]: Right tympanic membrane perforationFrom the collection of Dr Richard Buckingham [Citation ends]. [Figure caption and citation for the preceding image starts]: Left ear with effusion behind intact tympanic membraneFrom the collection of Dr Richard Buckingham [Citation ends].
[Figure caption and citation for the preceding image starts]: Left ear with effusion behind intact tympanic membraneFrom the collection of Dr Richard Buckingham [Citation ends].
Otitis media with effusion (OME) can follow acute middle-ear infection, upper respiratory tract infection, or recent airplane travel. Fluid can be seen behind the tympanic membrane, and will usually be reabsorbed. There are no signs or symptoms of acute inflammation.
Patients with recurring or chronic ear infections can develop cholesteatoma. These are formed from keratinizing squamous epithelium. They can be congenital, but are often acquired following tympanic membrane damage. If left untreated, they may erode into the ear ossicles and mastoid bone, and subsequently cause lateral sinus thrombosis, facial nerve paralysis, or even a brain abscess.[Figure caption and citation for the preceding image starts]: Right attic cholesteatomaFrom the collection of Dr Richard Buckingham [Citation ends].

Tumors
Fortunately, middle-ear tumors and neoplasms are rare. The most common middle-ear tumor is a vascular glomus tumor. It most commonly presents with pulsatile tinnitus followed by hearing loss.[26][27][Figure caption and citation for the preceding image starts]: Right ear with glomus tumor visible inferiorly behind intact tympanic membraneFrom the collection of Dr Richard Buckingham [Citation ends].

Trauma
Trauma to the ear and the temporal bone causes hearing loss in approximately 24% of patients.[28] Acutely, these patients may present with a hemotympanum. The blood is absorbed slowly over several weeks. As the blood is absorbed, the hearing usually improves. If the hearing does not improve, then the hearing loss may be due to ossicular discontinuity or fracture or inner-ear injury.
Perforation of the tympanic membrane may result from direct trauma to the temporal region, use of cotton buds, middle-ear infection, barotrauma from changes in atmospheric pressure (usually from scuba diving), and iatrogenically if the membrane does not heal following removal of drainage tubes.
Eustachian tube dysfunction
Occurs when the tube becomes blocked and air pressure cannot equalize. This may follow a cold or accompany symptoms of allergic rhinitis.
Congenital
Congenital hearing loss may follow any developmental anomalies of the ossicle chain. The stapes is most commonly affected because it requires the longest time for development.
Otosclerosis
Otosclerosis is one of the most common causes of acquired hearing loss and has both genetic and environmental causes. Patients usually present with a gradual unilateral or bilateral conductive hearing loss. Abnormal bone growth at the foot of the stapes restricts movement of the stapes and decreases the amount of sound transmitted to the cochlea. The exact cause for this is unknown, although viral and hereditary triggers have been suggested.[29]
Bone disease
Paget disease of the bone can directly affect the mobility of the ossicular chain with the formation of new bone.
Osteogenesis imperfecta can lead to fractures of the ear ossicles and hearing loss.
Inner ear
Patients who present with hearing loss located in the inner ear and/or central auditory pathways usually have a normal ear canal and tympanic membrane. The most common causes of acquired hearing impairment in adults are age (presbycusis) and noise.[30] Presbycusis is age-related, usually affects both ears, and is gradually progressive. Despite its high prevalence, presbyacusis is often underdiagnosed.[31]
Ototoxic drugs
Certain drugs are known to be ototoxic. Although hearing loss is usually reversible if the drug is stopped early, if continued, hearing loss can become permanent. Aminoglycoside antibiotics, such as gentamicin and amikacin, are ototoxic in a dose-dependent manner. Other medications that may cause ototoxicity include loop diuretics (in high dose), salicylates, antimalarial drugs, and cytotoxic agents, such as cisplatin.[32] Hearing loss usually begins at high frequencies.
Local infection/inflammation
Labyrinthitis refers to inflammation of the labyrinth; patients usually present with a sudden hearing loss.[33] Associated symptoms can include tinnitus, a feeling of pressure in the ear, and vertigo.
Meniere disease
Meniere disease mimics labyrinthitis with unilateral fluctuating hearing loss, tinnitus, a feeling of pressure in the ear, and vertigo. However, the symptoms are recurrent and an otolaryngology referral is indicated.[33][34]
Trauma
Temporal bone fractures seldom occur as isolated injuries. Approximately 12% of head injuries result in a fracture of the skull base, and up to 40% of these involve the temporal bone.[35] Temporal bone fractures can present with otorrhea of blood or cerebrospinal fluid, hearing loss (conductive or sensorineural), dizziness or vertigo, and facial paralysis.[28][36][37]
Noise-related hearing loss is one of the most common causes of acquired hearing loss in adults. It may result from working in a noisy environment, use of power tools, riding motorcycles, or recreational shooting.
Tumors
Lesions of the cochleovestibular nerve, such as vestibular schwannoma (acoustic neuroma), usually present with unilateral hearing loss, tinnitus, and imbalance.[33] It is recommended that all patients with unilateral aural symptoms, such as unilateral tinnitus and/or unilateral sudden sensorineural hearing loss, undergo magnetic resonance imaging to assess for retrocochlear pathology. Patients with vestibular schwannoma may experience hearing loss that improves or resolves with time.[38] The cardinal sign of neurofibromatosis type 2 is bilateral vestibular schwannomas.
Congenital
Congenital infections, such as cytomegalovirus (CMV), toxoplasmosis, and syphilis, can cause sensorineural deafness by damaging the cochlea. CMV is the most common cause of intrauterine infection and is a leading cause of sensorineural deafness.[39][40][41] Hearing loss tends to be delayed but progressive. Sensorineural deafness caused by congenital syphilis may be prevented by treatment within the first 3 months, although the evidence to support this is sparse.[42][43][44]
Hereditary causes are often a result of autosomal-recessive gene defects, so parents of an affected child may have normal hearing (e.g., abnormal expression of the GJB2 [connexin 26, Cx26] gene). More than 200 genes have been identified that can result in variable degrees of inner ear hearing loss.[45]
Enlargement of the vestibular aqueduct leads to progressive hearing loss in one third of patients with this temporal bone anomaly.[46]
There are several syndromes, such as Alport, Jervell Lange-Nielsen, and Waardenburg syndromes, that may include hearing loss as a feature. Alport syndrome is usually X linked and presents with glomerulonephritis, renal failure, and hearing loss. Jervell Lange-Nielsen syndrome is an autosomal-recessive disorder; a long QT syndrome presenting with arrhythmias, syncope, and sometimes sudden death. Hearing loss is a prominent feature of Waardenburg syndrome, a rare autosomal-dominant disorder. Other features include hypertelorism, a forelock of white hair, and patches of hypopigmented skin.
Neonatal jaundice can result in hearing loss owing to the neurotoxic effects of high levels of unconjugated bilirubin.[47][48] Babies most at risk are severely jaundiced (requiring an exchange transfusion), have a low birth weight, or are premature.
Neurologic
Multiple sclerosis (MS) may result in deafness by affecting the transmission of impulses down the vestibulocochlear nerve by demyelination
Stroke and vertebral artery dissection can result in ischemia and present with hearing loss.
Arnold-Chiari malformation may result in stretching of the nerve as the cerebellar tonsils descend and affect the transmission of sound impulses.
Acquired infections, such as meningitis, especially pneumococcal infection, can damage the inner-ear structures directly by direct invasion and by the inflammation caused by stimulation of the host response. Hearing loss may be temporary or permanent and can affect one third of patients with bacterial meningitis.[49]
Auditory neuropathy is a relatively rare form of hearing loss that primarily affects children in whom cochlear function is normal, but transmission to higher centers of hearing is unsuccessful. Diagnosis is based on a normal cochlear microphonic (or normal otoacoustic emissions) with an abnormal auditory brainstem response. Speech understanding is typically worse than expected for the level of hearing loss as determined by an audiogram.[50]
Systemic disease
Diabetes mellitus has been associated with higher rates of hearing impairment; the mechanism is unclear but may be due to effects on small blood vessels and nerves of the inner-ear structures.[51]
Sensorineural hearing loss is also a recognized feature of systemic lupus erythematosus (SLE) and granulomatosis with polyangiitis (formerly known as Wegener granulomatosis).
SLE can cause sudden hearing loss.[52]
Autoimmune inner-ear disease
In the absence of other autoimmune conditions, the inner ear can be the lone site of an autoimmune reaction leading to hearing loss that may recover with steroids. Laboratory tests are available, but their usefulness has not been demonstrated.[53]
Perilymphatic fistula
A perilymphatic fistula is an abnormal connection between the middle and inner ear. It is characterized by episodic dizziness, vertigo, and sudden hearing loss. This may be found in conjunction with congenital middle-ear abnormalities, as a result of trauma, or after surgery, typically on the stapes.
Idiopathic
90% of patients with sudden sensorineural hearing loss have no identifiable cause, even after adequate investigation.[2]
Use of this content is subject to our disclaimer