Approach
The difficulty in tricyclic antidepressant (TCA) overdose is that other conditions present with similar signs and symptoms. The constellation of decreased mental status, tachycardia, and hypotension may be due to sepsis, overdose of other medications (e.g., antihistamines) or substances (ethanol), or possibly a pulmonary embolus. Anticholinergic signs typical of TCA overdose may also be present in other types of overdose (e.g., diphenhydramine). After a short asymptomatic period, usually of less than 1 to 2 hours, a rapid decline follows in both mental and cardiovascular status. Some patients present in varying states of consciousness so that a history of overdose cannot be obtained.
The steps to diagnosis are, therefore, as follows: after ensuring adequate airway, breathing, and circulation, the patient should be attached to a cardiac monitor. Intravenous access should be obtained and an ECG performed as soon as the patient is stabilized on arrival, as this is the most helpful tool for determining the presence of TCA toxicity.
Arterial blood gas analysis should be performed if ingestion of a potentially toxic dose is suspected, to determine if the patient is acidotic. Any acidosis is detrimental since it increases cardiotoxicity.
Clinical features
Clinical features suggestive of TCA toxicity include:
Anticholinergic symptoms, such as dry, flushed skin, dilated pupils, absent bowel sounds, or urinary retention
Impaired consciousness level
Tachycardia
Hypotension
Arrhythmias
Seizures
Other variable clinical signs include: divergent squint, internuclear ophthalmoplegia and gaze paralysis, nystagmus, and myoclonic and choreoathetoid movements. Increased muscle tone, hyperreflexia, and extensor plantar responses may occur.
Features of serotonin toxicity may also occur if the patient has coingested other drugs that increase the effect of serotonin, or is taking one of these drugs therapeutically. These include: selective serotonin reuptake inhibitors (SSRIs), venlafaxine, monoamine oxidase inhibitors, amphetamines, cocaine, MDMA (ecstasy), linezolid, tramadol, or triptans. The clinical features of serotonin syndrome include hyperpyrexia, impaired consciousness level or agitation, increased muscle tone, and clonus. It is often associated with an elevated creatine kinase level.[13]
Investigations
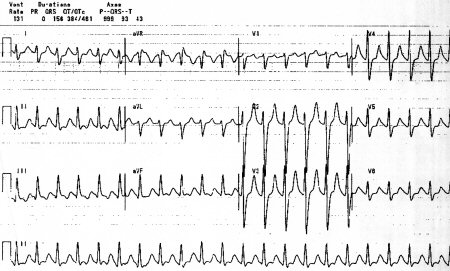
ECG features are helpful for determining the presence of TCA toxicity:[17]
Sinus tachycardia is commonly seen.
QRS duration >100 milliseconds is often present in TCA toxicity, but its absence does not exclude the diagnosis.
Confirming the presence of a terminal 40 milliseconds rightward axis shift, seen as an R-wave deflection in aVR or an S wave in I or aVL, is useful for diagnosing TCA overdose.[18] Absence of this rightward axis shift makes the diagnosis less likely, and other causes should be considered, including overdose of other medications and nontoxicological causes.
QRS prolongation >100 milliseconds indicates a 30% likelihood of seizure. When the QRS prolongs to >160 milliseconds there is a 50% risk of arrhythmia.[19][Figure caption and citation for the preceding image starts]: Classic ECG changesFrom the collection of R.S. Hoffman; used with permission [Citation ends].
Other ECG changes that can occur in TCA poisoning include:
Prolonged QTc duration
Prolonged PR interval
AV block
Non-specific ST and T wave changes
Downward sloping ST elevation in leads V1 to V3 with right bundle branch block (Brugada wave).[17]
Any condition that causes right heart strain, such as bronchospasm or large pulmonary embolus, may cause a similar ECG pattern.
If QRS prolongation is found on ECG, a cardiac monitor should be attached to the patient and repeat 12-lead ECGs should be performed at least every hour for the first 6 hours. Once QRS prolongation is confirmed, a bolus of sodium bicarbonate can be given as a therapeutic trial. If the duration of the QRS narrows this confirms the presence of a sodium channel blocker, although not specifically a TCA.
Serum TCA levels can be obtained but are not as valuable as an ECG.[19] These levels are not rapidly available and should never be used to guide management in the setting of an acute TCA overdose. Urine TCA screens are available more rapidly, but their clinical usefulness is limited in the management of an overdose. However, it may assist when there is a strong suspicion of a significant co-ingestion.
Use of this content is subject to our disclaimer