Differentials
Kawasaki disease
SIGNS / SYMPTOMS
Uncommon in children >8 years.[3]
Prominent features are fever lasting 5 days or more, conjunctivitis, erythematous changes of the mouth or oral cavity and/or cracking of the lips, polymorphous rash, cervical lymphadenopathy, and edema and/or erythema of extremities.
INVESTIGATIONS
Diagnosis is clinical.
Suggestive laboratory and diagnostic imaging findings include elevated inflammatory markers (CRP, erythrocyte sedimentation rate), sterile pyuria, anemia, thrombocytosis, leukocytosis, hypoalbuminemia, hepatitis, cerebrospinal fluid pleocytosis, pericardial effusion, gallbladder hydrops, and coronary artery abnormalities.
Erythema infectiosum (parvovirus B19, fifth disease)
SIGNS / SYMPTOMS
Mild systemic symptoms and/or fever are followed in 7-10 days by a distinctive erythematous facial rash with a slapped cheek appearance.[3]
Patients may develop a second macular, lacy, diffuse rash on the trunk and extremities after facial rash.[3]
[Figure caption and citation for the preceding image starts]: Typical erythematous "slapped cheeks" of erythema infectiosumFrom the collection of Gary A. Dyer, MD; used with permission [Citation ends].
Rubella
SIGNS / SYMPTOMS
Presence of lymphadenopathy typically in posterior auricular or suboccipital chains.[3]
Cough and conjunctivitis are common.
[Figure caption and citation for the preceding image starts]: Rubella presenting as a generalized abdominal rashCourtesy of the CDC Public Health Image Library [Citation ends].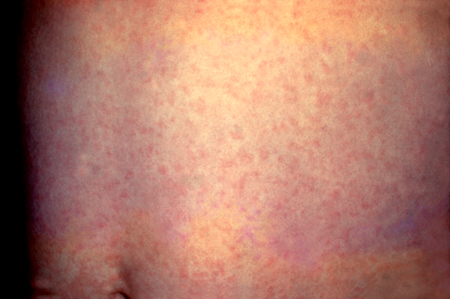
INVESTIGATIONS
Detection of rubella IgM antibodies in acute serum; or a fourfold or greater increase in antibody titer between acute and convalescent periods or seroconversion between acute and convalescent IgG serum titers.[3]
Reverse transcriptase-polymerase chain reaction from throat or nasopharyngeal swab: positive for rubella virus.[3]
Measles (rubeola)
SIGNS / SYMPTOMS
More common in infants age <1 year, and in older adolescents and adults not previously vaccinated against measles.[3]
A pathognomonic enanthem consisting of gray-white papules on the buccal mucosa (Koplik spots) occurs early in the disease. The measles rash spreads from the head and neck downward.
Cough, coryza, and conjunctivitis are common.[3]
History of travel to countries where measles is still endemic (in Africa, Asia) or where large outbreaks have occurred.[37]
[Figure caption and citation for the preceding image starts]: Koplik spotsCDC Public Health Image Library [Citation ends].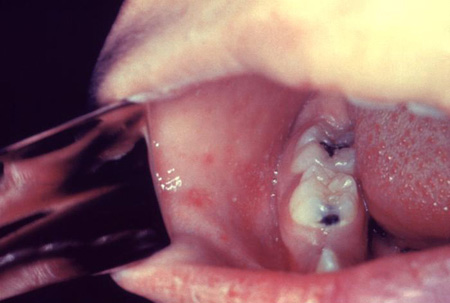
INVESTIGATIONS
Detection of measles IgM antibodies in acute serum; a fourfold rise in measles IgG antibody concentration in paired acute and convalescent serum specimens (collected 10 days apart).[3]
Reverse transcriptase-polymerase chain reaction from one or more of the following sites - blood, throat/nasal/oropharyngeal swab, bronchoalveolar (BAL) lavage fluid or urine: positive for measles virus.[3]
Infectious mononucleosis (Epstein-Barr virus [EBV], glandular fever)
SIGNS / SYMPTOMS
A polymorphous rash, usually on the trunk and arms, may appear later in the course of the disease in up to 20% of patients (more common in patients who have received amoxicillin with acute illness).[3]
Lymphadenopathy may be more diffuse.
Enteroviral infection
SIGNS / SYMPTOMS
Most common in summer and early autumn.[3]
Presence of a rash involving palms and soles; typically papular or vesicular.
Enanthem of ulcers or vesicles (without petechiae).[3]
Respiratory (cough, rhinorrhea) or gastrointestinal symptoms (vomiting, diarrhea, abdominal pain) are common.[3]
[Figure caption and citation for the preceding image starts]: Close-up of a vesicle on the hand of a 3-year-old boy with hand-foot-and-mouth disease.Dr P. Marazzi/Science Photo Library [Citation ends].
INVESTIGATIONS
Reverse transcriptase-polymerase chain reaction from body fluids (including nasopharyngeal or throat swab, vesicle fluid, blood, urine, stool, and cerebrospinal fluid): positive for enterovirus.[3]
Rat-bite fever (Streptobacillus moniliformis infection)
Staphylococcal toxic shock syndrome
SIGNS / SYMPTOMS
Diffuse erythroderma of the skin and mucous membranes, particularly of the palms and soles.
Recent use of tampons in menstruating women.
Patients may present with acute mental status changes (confusion, agitation, and change in level of consciousness).
Myocarditis, peritonitis, and endophthalmitis may be present.
Hypotension and shock usually develop 4-8 hours following hospital admission.
[Figure caption and citation for the preceding image starts]: Rash and subcutaneous edema of the right hand due to toxic shock syndromeFrom the CDC and the Public Health Image Library [Citation ends].
INVESTIGATIONS
Blood, wound, fluid, or tissue culture positive for Staphylococcus aureus.
Cutaneous drug reactions
SIGNS / SYMPTOMS
History of recent medication or drug ingestion.
[Figure caption and citation for the preceding image starts]: Drug exanthem due to phenytoinPhotography courtesy of Brian L. Swick [Citation ends].
INVESTIGATIONS
Clinical diagnosis; no differentiating tests.
Arcanobacterium haemolyticum
SIGNS / SYMPTOMS
No differentiating signs and symptoms.
More common in adolescents ages 15-18 years.[38]
INVESTIGATIONS
Throat culture positive for Arcanobacterium haemolyticum.
Staphylococcal scalded skin syndrome
SIGNS / SYMPTOMS
Localized bullous impetigo is present. The hallmark is the toxin-mediated cleavage of the stratum granulosum layer of the epidermis (i.e., Nikolsky sign).[3]
INVESTIGATIONS
Isolation of Staphylococcus aureus from culture of otherwise sterile body fluid. Detection of S aureus from blood cultures growing gram-positive organisms via molecular assays.[3]
Use of this content is subject to our disclaimer