History and physical examination form the initial approach in the evaluation of a patient with possible appendicitis. It is routine practice in the US to request a computed tomography (CT) scan for patients presenting to the emergency room with features of acute appendicitis.[29]Bendeck SE, Nino-Murcia M, Berry GJ, et al. Imaging for suspected appendicitis: negative appendectomy and perforation rates. Radiology. 2002 Oct;225(1):131-6.
http://www.ncbi.nlm.nih.gov/pubmed/12354996?tool=bestpractice.com
Validated clinical decision tools such as the Alvarado score demonstrate high sensitivities and are useful for excluding appendicitis, but lack specificity.[30]Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986 May;15(5):557-64.
http://www.ncbi.nlm.nih.gov/pubmed/3963537?tool=bestpractice.com
[31]Kularatna M, Lauti M, Haran C, et al. Clinical prediction rules for appendicitis in adults: which is best? World J Surg. 2017 Jul;41(7):1769-81.
http://www.ncbi.nlm.nih.gov/pubmed/28258458?tool=bestpractice.com
[32]Frountzas M, Stergios K, Kopsini D, et al. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int J Surg. 2018 Aug;56:307-14.
http://www.ncbi.nlm.nih.gov/pubmed/30017607?tool=bestpractice.com
Ultrasound or magnetic resonance imaging (MRI) of the abdomen are recommended if the patient is pregnant.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
[33]American College of Radiology. ACR appropriateness criteria: right lower quadrant pain - suspected appendicitis. 2022 [internet publication].
https://acsearch.acr.org/docs/69357/Narrative
Women of childbearing age should have a pelvic examination to rule out other pelvic pathology.[34]Basaran A, Basaran M. Diagnosis of acute appendicitis during pregnancy: a systematic review. Obstet Gynecol Surv. 2009 Jul;64(7):481-8; quiz 499.
http://www.ncbi.nlm.nih.gov/pubmed/19545456?tool=bestpractice.com
History
The typical picture of central pain migrating to the right iliac fossa, associated with nausea, vomiting, and anorexia, occurs in less than half of presentations.[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
Abdominal pain is the most common presenting symptom. Pain typically starts at the mid-abdominal region and 1-12 hours later shifts to the right lower quadrant as the inflammation progresses.[36]Lee SL, Walsh AJ, Ho HS. Computed tomography and ultrasonography do not improve and may delay the diagnosis and treatment of acute appendicitis. Arch Surg. 2001 May;136(5):556-62.
https://jamanetwork.com/journals/jamasurgery/fullarticle/391421
http://www.ncbi.nlm.nih.gov/pubmed/11343547?tool=bestpractice.com
Pain tends to be constant in nature, with intermittent abdominal cramps, and is usually worse on movement and coughing.
Location of the pain may vary depending upon the position of the appendix:[37]Lewis SR, Mahony PJ, Simpson J. Appendicitis. BMJ. 2011 Oct 6;343:d5976.
http://www.ncbi.nlm.nih.gov/pubmed/21980077?tool=bestpractice.com
Retrocecal appendix may cause flank or back pain
Retroileal appendix may cause testicular pain due to irritation of the spermatic artery or ureter
Pelvic appendix may cause suprapubic pain
A long appendix with tip inflammation in the left lower quadrant may cause pain to that region.
Anorexia is almost always present.[12]Snyder MJ, Guthrie M, Cagle S. Acute appendicitis: efficient diagnosis and management. Am Fam Physician. 2018 Jul 1;98(1):25-33.
https://www.aafp.org/afp/2018/0701/p25.html
http://www.ncbi.nlm.nih.gov/pubmed/30215950?tool=bestpractice.com
If the patient is hungry and wants to eat, this is reassuring and makes appendicitis less likely.[37]Lewis SR, Mahony PJ, Simpson J. Appendicitis. BMJ. 2011 Oct 6;343:d5976.
http://www.ncbi.nlm.nih.gov/pubmed/21980077?tool=bestpractice.com
Nausea and vomiting are usually present in 75% of patients.[12]Snyder MJ, Guthrie M, Cagle S. Acute appendicitis: efficient diagnosis and management. Am Fam Physician. 2018 Jul 1;98(1):25-33.
https://www.aafp.org/afp/2018/0701/p25.html
http://www.ncbi.nlm.nih.gov/pubmed/30215950?tool=bestpractice.com
Absolute constipation is a late feature.[38]Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10(3):115-9.
https://www.sciencedirect.com/science/article/pii/S1743919112000246?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/22349155?tool=bestpractice.com
Features that are significantly associated with appendicitis in pregnant patients are nausea, vomiting, and local peritonitis.[39]Brown JJ, Wilson C, Coleman S, Joypaul BV. Appendicitis in pregnancy: an ongoing diagnostic dilemma. Colorectal Dis. 2009 Feb;11(2):116-22.
http://www.ncbi.nlm.nih.gov/pubmed/18513191?tool=bestpractice.com
Complicated appendicitis (perforation or intra-abdominal abscess) is more likely the greater the duration of symptoms and in older patients (>50 years).[40]Temple CL, Shirley AH, Temple WJ. The natural history of appendicitis in adults. A prospective study. Ann Surg. 1995 Mar;221(3):278-81.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1234570/pdf/annsurg00049-0078.pdf
http://www.ncbi.nlm.nih.gov/pubmed/7717781?tool=bestpractice.com
[41]Franz MG, Norman J, Fabri PJ. Increased morbidity of appendicitis with advancing age. Am Surg. 1995 Jan;61(1):40-4.
http://www.ncbi.nlm.nih.gov/pubmed/7832380?tool=bestpractice.com
Children may present with nonspecific abdominal pain, anorexia, and vomiting.[8]Davenport M. Acute abdominal pain in children. BMJ. 1996 Feb 24;312(7029):498-501.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2349926
http://www.ncbi.nlm.nih.gov/pubmed/8597689?tool=bestpractice.com
Physical exam
Usually, there are no significant changes in vital signs. Patients may have a low-grade fever.[2]Moris D, Paulson EK, Pappas TN. Diagnosis and management of acute appendicitis in adults: A Review. JAMA. 2021 Dec 14;326(22):2299-311.
http://www.ncbi.nlm.nih.gov/pubmed/34905026?tool=bestpractice.com
[37]Lewis SR, Mahony PJ, Simpson J. Appendicitis. BMJ. 2011 Oct 6;343:d5976.
http://www.ncbi.nlm.nih.gov/pubmed/21980077?tool=bestpractice.com
In patients presenting with a high-grade fever, another diagnosis should be considered.[2]Moris D, Paulson EK, Pappas TN. Diagnosis and management of acute appendicitis in adults: A Review. JAMA. 2021 Dec 14;326(22):2299-311.
http://www.ncbi.nlm.nih.gov/pubmed/34905026?tool=bestpractice.com
Tachycardia may be present (but this can also indicate a perforated appendix).[42]Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006 Sep 9;333(7567):530-4.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1562475
http://www.ncbi.nlm.nih.gov/pubmed/16960208?tool=bestpractice.com
A classic sign is right lower quadrant abdominal tenderness (McBurney sign) and localized rebound tenderness, if appendix is anterior. There may also be pain in the right lower quadrant after compressing the left lower quadrant (Rovsing sign).[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
In retrocecal appendicitis, pain may be elicited in the right lower quadrant with the patient lying on their left side and slowly extending the right thigh to cause a stretch in the iliopsoas muscle (psoas sign) or by internal rotation of the flexed right thigh (obturator sign).[12]Snyder MJ, Guthrie M, Cagle S. Acute appendicitis: efficient diagnosis and management. Am Fam Physician. 2018 Jul 1;98(1):25-33.
https://www.aafp.org/afp/2018/0701/p25.html
http://www.ncbi.nlm.nih.gov/pubmed/30215950?tool=bestpractice.com
However, Rovsing and obturator signs are of limited diagnostic value for acute appendicitis.[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
[38]Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10(3):115-9.
https://www.sciencedirect.com/science/article/pii/S1743919112000246?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/22349155?tool=bestpractice.com
[43]Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of acute appendicitis. Br J Surg. 2004 Jan;91(1):28-37.
http://www.ncbi.nlm.nih.gov/pubmed/14716790?tool=bestpractice.com
Classic abdominal findings may not be present if the appendix is in an atypical position.[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
Patients with perforation may present acutely ill with hypotension, tachycardia, and a tense, distended abdomen with generalized guarding and absent bowel sounds.[37]Lewis SR, Mahony PJ, Simpson J. Appendicitis. BMJ. 2011 Oct 6;343:d5976.
http://www.ncbi.nlm.nih.gov/pubmed/21980077?tool=bestpractice.com
A palpable mass may be felt with appendiceal perforation that has been contained by the omentum, resulting in a periappendiceal abscess.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
In children, pain with coughing and hopping can support the diagnosis.[9]Benabbas R, Hanna M, Shah J, et al. Diagnostic accuracy of history, physical examination, laboratory tests, and point-of-care ultrasound for pediatric acute appendicitis in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2017 May;24(5):523-51.
https://onlinelibrary.wiley.com/doi/full/10.1111/acem.13181
http://www.ncbi.nlm.nih.gov/pubmed/28214369?tool=bestpractice.com
Analgesia may be useful to facilitate abdominal exam if pain limits the examination. Analgesia does not lead to missed diagnoses in children.[44]Green R, Bulloch B, Kabani A, et al. Early analgesia for children with acute abdominal pain. Pediatrics. 2005 Oct;116(4):978-83.
http://www.ncbi.nlm.nih.gov/pubmed/16199711?tool=bestpractice.com
[45]Manterola C, Vial M, Moraga J, et al. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD005660.
https://www.doi.org/10.1002/14651858.CD005660.pub3
http://www.ncbi.nlm.nih.gov/pubmed/21249672?tool=bestpractice.com
See Evaluation of abdominal pain in children.
The diagnosis of appendicitis in pregnant women should not be made based on history and exam only. Blood tests, including inflammatory markers, should be ordered.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
Appendicitis is the most common nonobstetric surgical condition during pregnancy.[46]Carstens AK, Fensby L, Penninga L. Nonoperative treatment of appendicitis during pregnancy in a remote area. AJP Rep. 2018 Jan;8(1):e37-8.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5830160
http://www.ncbi.nlm.nih.gov/pubmed/29497573?tool=bestpractice.com
A delay in diagnosis and treatment may result in perforation, which is associated with significant maternal and fetal mortality.[46]Carstens AK, Fensby L, Penninga L. Nonoperative treatment of appendicitis during pregnancy in a remote area. AJP Rep. 2018 Jan;8(1):e37-8.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5830160
http://www.ncbi.nlm.nih.gov/pubmed/29497573?tool=bestpractice.com
In pregnant women, atypical pain such as right upper quadrant or right flank pain may occur after the first trimester due to displacement of the appendix by the gravid uterus.[42]Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006 Sep 9;333(7567):530-4.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1562475
http://www.ncbi.nlm.nih.gov/pubmed/16960208?tool=bestpractice.com
A collateral history should be taken if communication presents a challenge (e.g., when there is a language barrier, or in patients who are very young, have dementia, have a mental health diagnosis, or have a learning difficulty).[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
Appendicitis should be suspected if there is a history of becoming withdrawn or less active, or having reduced oral intake.[35]Baird DLH, Simillis C, Kontovounisios C, et al. Acute appendicitis. BMJ. 2017 Apr 19;357:j1703.
https://spiral.imperial.ac.uk/bitstream/10044/1/48493/2/bmj.j1703.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/28424152?tool=bestpractice.com
Investigations
Blood tests
All patients with abdominal discomfort should have a complete blood count taken. Mild leukocytosis (10,000-18,000/microliter) with increased neutrophils is usually present. In children, CRP level on admission ≥10 mg/L and leukocytosis ≥16,000/microliter are strong predictive factors for appendicitis.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
Imaging
Some form of imaging is usually warranted. Most nonpregnant patients presenting to the emergency room with abdominal pain suggestive of appendicitis will have a CT scan of the abdomen and pelvis.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
[33]American College of Radiology. ACR appropriateness criteria: right lower quadrant pain - suspected appendicitis. 2022 [internet publication].
https://acsearch.acr.org/docs/69357/Narrative
Preoperative imaging with a CT scan of the abdomen (ultrasound or MRI for pregnant women) now forms the usual standard of care. Women and children, in particular, may benefit from preoperative imaging.[9]Benabbas R, Hanna M, Shah J, et al. Diagnostic accuracy of history, physical examination, laboratory tests, and point-of-care ultrasound for pediatric acute appendicitis in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2017 May;24(5):523-51.
https://onlinelibrary.wiley.com/doi/full/10.1111/acem.13181
http://www.ncbi.nlm.nih.gov/pubmed/28214369?tool=bestpractice.com
[29]Bendeck SE, Nino-Murcia M, Berry GJ, et al. Imaging for suspected appendicitis: negative appendectomy and perforation rates. Radiology. 2002 Oct;225(1):131-6.
http://www.ncbi.nlm.nih.gov/pubmed/12354996?tool=bestpractice.com
[47]Bachur RG, Callahan MJ, Monuteaux MC, et al. Integration of ultrasound findings and a clinical score in the diagnostic evaluation of pediatric appendicitis. J Pediatr. 2015 May;166(5):1134-9.
http://www.ncbi.nlm.nih.gov/pubmed/25708690?tool=bestpractice.com
Choice of imaging modality
Although CT scan has greater sensitivity and specificity than ultrasound in diagnosing appendicitis, the latter is readily available, rapid, and able to be performed at the bedside.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
[48]Terasawa T, Blackmore CC, Bent S, et al. Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Ann Intern Med. 2004 Oct 5;141(7):537-46.
http://www.ncbi.nlm.nih.gov/pubmed/15466771?tool=bestpractice.com
[49]Dahabreh IJ, Adam GP, Halladay CW, et al. Diagnosis of right lower quadrant pain and suspected acute appendicitis. In: Agency for Healthcare Research and Quality (US). AHRQ Comparative effectiveness reviews report no. 15(16)-EHC025-EF. 2015. Rockville, MD: Agency for Healthcare Research and Quality (US).
https://www.ncbi.nlm.nih.gov/books/NBK355441
http://www.ncbi.nlm.nih.gov/pubmed/27054223?tool=bestpractice.com
[50]Kumar SS, Collings AT, Lamm R, et al. SAGES guideline for the diagnosis and treatment of appendicitis. Surg Endosc. 2024 Jun;38(6):2974-94.
http://www.ncbi.nlm.nih.gov/pubmed/38740595?tool=bestpractice.com
Ultrasound has a sensitivity of 71% to 94% and specificity of 60% to 98% for acute appendicitis; if ultrasound is unequivocally positive for appendicitis, ultrasound has comparable accuracy to a positive CT or MRI for ruling in appendicitis.[51]Fu J, Zhou X, Chen L, et al. Abdominal ultrasound and its diagnostic accuracy in diagnosing acute appendicitis: a meta-analysis. Front Surg. 2021 Jun 28:8:707160.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8273278
http://www.ncbi.nlm.nih.gov/pubmed/34262936?tool=bestpractice.com
[52]American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Appendicitis, Diercks DB, Adkins EJ, et al. Clinical policy: critical issues in the evaluation and management of emergency department patients with suspected appendicitis: approved by ACEP Board of Directors February 1, 2023. Ann Emerg Med. 2023 Jun;81(6):e115-52.
https://www.annemergmed.com/article/S0196-0644(23)00029-X/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/37210169?tool=bestpractice.com
If, on ultrasound, a normal appendix is visualized in its full length, then acute appendicitis can be excluded. However, this is rarely the case, and the greatest utility for ultrasound is to detect an alternative cause of abdominal pain that excludes appendicitis.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
Appendiceal CT scan is increasingly used as the initial diagnostic test for acute appendicitis, and it is routine practice in the US to request a CT for patients presenting to the emergency room with features of acute appendicitis.[29]Bendeck SE, Nino-Murcia M, Berry GJ, et al. Imaging for suspected appendicitis: negative appendectomy and perforation rates. Radiology. 2002 Oct;225(1):131-6.
http://www.ncbi.nlm.nih.gov/pubmed/12354996?tool=bestpractice.com
The Infectious Diseases Society of America (IDSA) offers a conditional recommendation for abdominal CT as the initial imaging modality to diagnose acute appendicitis.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
A CT is also indicated in atypical presentations.[33]American College of Radiology. ACR appropriateness criteria: right lower quadrant pain - suspected appendicitis. 2022 [internet publication].
https://acsearch.acr.org/docs/69357/Narrative
[54]American College of Radiology. ACR appropriateness criteria: acute nonlocalized abdominal pain. 2018 [internet publication].
https://acsearch.acr.org/docs/69467/Narrative
However, delayed surgery subsequent to CT scan for presumed appendicitis is associated with an increased rate of appendiceal perforation.[55]Musunuru S, Chen H, Rikkers LF, et al. Computed tomography in the diagnosis of acute appendicitis: definitive or detrimental? J Gastrointest Surg. 2007 Nov;11(11):1417-21; discussion 1421-2.
http://www.ncbi.nlm.nih.gov/pubmed/17701439?tool=bestpractice.com
Intravenous contrast is usually appropriate whenever a CT is obtained in adults with suspected acute appendicitis; however, CT without intravenous contrast also has high diagnostic accuracy in detecting acute appendicitis and may be appropriate.[33]American College of Radiology. ACR appropriateness criteria: right lower quadrant pain - suspected appendicitis. 2022 [internet publication].
https://acsearch.acr.org/docs/69357/Narrative
[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
Intravenous contrast-enhanced CT scan with or without oral contrast has up to 100% sensitivity compared with 92% sensitivity in nonintravenous contrast-enhanced CT scan.[56]Chiu YH, Chen JD, Wang SH, et al. Whether intravenous contrast is necessary for CT diagnosis of acute appendicitis in adult ED patients? Acad Radiol. 2013 Jan;20(1):73-8.
https://www.academicradiology.org/article/S1076-6332(12)00385-6/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/22951113?tool=bestpractice.com
[57]Hlibczuk V, Dattaro JA, Jin Z, et al. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med. 2010 Jan;55(1):51-9.e1.
http://www.ncbi.nlm.nih.gov/pubmed/19733421?tool=bestpractice.com
[58]Arruzza E, Milanese S, Li LSK, et al. Diagnostic accuracy of computed tomography and ultrasound for the diagnosis of acute appendicitis: A systematic review and meta-analysis. Radiography (Lond). 2022 Nov;28(4):1127-41.
http://www.ncbi.nlm.nih.gov/pubmed/36130469?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: CT abdomen - thickened appendix.Nasim Ahmed, MBBS, FACS; used with permission [Citation ends].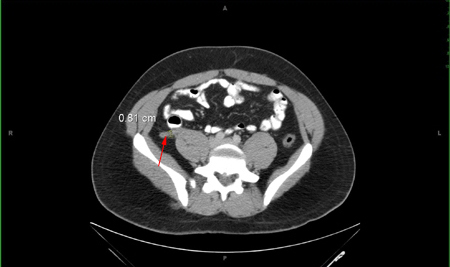 The IDSA recommends to consider observation and supportive care, with or without antibiotics, if CT is negative but clinical suspicion for acute appendicitis persists.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
If clinical suspicion is high, consider surgical intervention.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
Laparoscopy may also be reasonable if there is diagnostic uncertainty.
The IDSA recommends to consider observation and supportive care, with or without antibiotics, if CT is negative but clinical suspicion for acute appendicitis persists.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
If clinical suspicion is high, consider surgical intervention.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
Laparoscopy may also be reasonable if there is diagnostic uncertainty.
In pregnant women presenting with features of appendicitis, an abdominal sonogram should be performed to identify the appendix.[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
If the sonogram examination is inconclusive, an abdominal MRI (particularly in early pregnancy) may be appropriate.[33]American College of Radiology. ACR appropriateness criteria: right lower quadrant pain - suspected appendicitis. 2022 [internet publication].
https://acsearch.acr.org/docs/69357/Narrative
[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
[54]American College of Radiology. ACR appropriateness criteria: acute nonlocalized abdominal pain. 2018 [internet publication].
https://acsearch.acr.org/docs/69467/Narrative
MRI has been proven to be a highly accurate diagnostic test for acute appendicitis, with a sensitivity of 0.96 and specificity of 0.97 in pregnant women.[59]D'Souza N, Hicks G, Beable R, et al. Magnetic resonance imaging (MRI) for diagnosis of acute appendicitis. Cochrane Database Syst Rev. 2021 Dec 14;(12):CD012028.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD012028.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/34905621?tool=bestpractice.com
However, a negative or inconclusive MRI does not exclude appendicitis and surgery should still be considered if clinical suspicion is high.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
[59]D'Souza N, Hicks G, Beable R, et al. Magnetic resonance imaging (MRI) for diagnosis of acute appendicitis. Cochrane Database Syst Rev. 2021 Dec 14;(12):CD012028.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD012028.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/34905621?tool=bestpractice.com
In children, point-of-care ultrasound is the most appropriate first-line diagnostic tool, if an imaging investigation is indicated based on clinical assessment.[52]American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Appendicitis, Diercks DB, Adkins EJ, et al. Clinical policy: critical issues in the evaluation and management of emergency department patients with suspected appendicitis: approved by ACEP Board of Directors February 1, 2023. Ann Emerg Med. 2023 Jun;81(6):e115-52.
https://www.annemergmed.com/article/S0196-0644(23)00029-X/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/37210169?tool=bestpractice.com
[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
In children, if there is diagnostic doubt and ultrasound results are inconclusive, a second-line imaging technique (i.e., CT or MRI) should be used based on local availability and expertize.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
[53]Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis. 2024 Oct 4;79(supplement_3):S81-7.
https://academic.oup.com/cid/article/79/Supplement_3/S81/7706348
http://www.ncbi.nlm.nih.gov/pubmed/38965057?tool=bestpractice.com
Low-dose CT is preferred if ultrasound is negative.[7]Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020 Apr 15;15(1):27.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386163
http://www.ncbi.nlm.nih.gov/pubmed/32295644?tool=bestpractice.com
Tests to exclude other causes
A urinalysis should be performed to exclude possible urinary tract infection or renal colic. Sexually active women of childbearing age should have a urinary pregnancy test.
Novel biomarkers
Several novel biomarkers may be of value in the diagnosis and severity assessment of acute appendicitis. These are not routinely used or recommended in established guidelines, and require further investigation.
Neutrophil-to-lymphocyte ratio. The simple ratio between neutrophils and lymphocytes measured in peripheral blood has been shown to have moderate predictive power for acute appendicitis and may be a useful adjunctive tool for diagnosis.[61]Eun S, Ho IG, Bae GE, et al. Neutrophil-to-lymphocyte ratio for the diagnosis of pediatric acute appendicitis: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2021 Nov;25(22):7097-107.
https://www.europeanreview.org/article/27263
http://www.ncbi.nlm.nih.gov/pubmed/34859875?tool=bestpractice.com
Hyponatremia. Several studies have shown a link between hyponatremia and acute appendicitis, and as a predictor of complicated appendicitis.[62]Giannis D, Matenoglou E, Moris D. Hyponatremia as a marker of complicated appendicitis: A systematic review. Surgeon. 2020 Oct;18(5):295-304.
http://www.ncbi.nlm.nih.gov/pubmed/32035730?tool=bestpractice.com
[63]Zhan W, Deng W, Liu Y, et al. Hyponatremia as a predictor of complicated appendicitis in children: A systematic review and meta-analysis. Asian J Surg. 2022 Oct;45(10):2009-11.
https://www.sciencedirect.com/science/article/pii/S1015958422004493?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/35490069?tool=bestpractice.com
Pentraxin 3.[64]Anand S, Pakkasjärvi N, Bajpai M, et al. Utility of Pentraxin-3 as a biomarker for diagnosis of acute appendicitis: a systematic review and meta-analysis. Pediatr Surg Int. 2022 Aug;38(8):1105-12.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9259520
http://www.ncbi.nlm.nih.gov/pubmed/35704081?tool=bestpractice.com
Serum amyloid A. One systematic review and meta-analysis showed that serum amyloid A has a sensitivity and specificity for acute appendicitis of 0.87 and 0.74 respectively.[65]Shi W, Wu Y, Zhong L, et al. Diagnostic accuracy of serum amyloid A in acute appendicitis: a systematic review and meta-analysis. Surg Infect (Larchmt). 2022 May;23(4):380-7.
http://www.ncbi.nlm.nih.gov/pubmed/35319305?tool=bestpractice.com
Platelet indices. Studies suggest that low mean platelet volume is a marker of acute appendicitis.[66]Tullavardhana T, Sanguanlosit S, Chartkitchareon A. Role of platelet indices as a biomarker for the diagnosis of acute appendicitis and as a predictor of complicated appendicitis: a meta-analysis. Ann Med Surg (Lond). 2021 Jun;66:102448.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8181186
http://www.ncbi.nlm.nih.gov/pubmed/34136215?tool=bestpractice.com
[67]Shen G, Li S, Shao Z, et al. Platelet indices in patients with acute appendicitis: a systematic review with meta-analysis. Updates Surg. 2021 Aug;73(4):1327-41.
http://www.ncbi.nlm.nih.gov/pubmed/33439467?tool=bestpractice.com
