Differentials
Neoplasm (primary or metastatic lung cancer, lymphoma)
SIGNS / SYMPTOMS
Malignancy is associated with a low-grade fever, absence of leukocytosis, minimal systemic complaints, absence of factors that predispose to gastric content aspiration, no response to antibiotics within 10 days, and a deteriorating course.[29] Haemoptysis is commonly associated with bronchogenic carcinoma.
INVESTIGATIONS
Chest x-ray: less ground-glass infiltrate surrounding the cavity.
Sputum cytology: may show malignant cells.
CT chest and bronchoscopy: confirm the obstructing lesion.
[Figure caption and citation for the preceding image starts]: Chest x-ray showing a lung tumour with central cavitationFrom the collection of Dr Ioannis P. Kioumis [Citation ends].
Tuberculosis
SIGNS / SYMPTOMS
History of exposure to a tuberculosis-infected patient.
Systemic symptoms of fatigue, malaise, anorexia, and weight loss, as well as a low-grade fever with night sweats, are prominent.
INVESTIGATIONS
Chest x-ray: cavity is usually located in the upper lobes. [Figure caption and citation for the preceding image starts]: Chest x-ray showing an abscess-like cavitating lesion due to tuberculosisFrom the collection of Dr Ioannis P. Kioumis [Citation ends].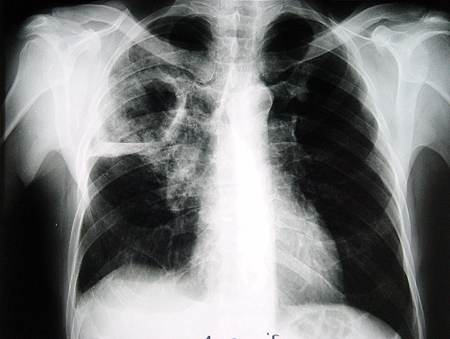
Sputum smear and culture in Lowenstein-Jensen media: positive for acid-fast bacilli.
CT chest: cavitating lesions typically in the upper lobes and usually accompanied by parenchymal infiltrates. Tree-in-bud pattern may be present.
Necrotising pneumonia
SIGNS / SYMPTOMS
Acute, often fulminant infection. Duration of illness before recognition is usually short. Causative organisms include Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas species.[38]
INVESTIGATIONS
Chest x-ray: multiple cavities are usually present. Pleural effusion and empyema are common findings.
Loculated empyema
SIGNS / SYMPTOMS
On respiratory exam, dullness to percussion, decreased breath sounds, and reduced vocal resonance are usually found.
INVESTIGATIONS
CT chest: empyema appears lenticular in shape, and has a thin wall with smooth luminal margins and a smooth exterior wall. It forms obtuse angles with the chest wall, and shows signs of compression of the uninvolved lung. Separate pleural layers are also seen.[34]
Fungal infection
SIGNS / SYMPTOMS
History of travel to or residence in an endemic area, or occupational exposure.
More prevalent in patients with impaired cell-mediated immunity (e.g., AIDS, transplant immunosuppression, malignancies) or granulocytopenia.
INVESTIGATIONS
Demonstration of typical yeast in fluid or tissue specimens.
Culture of pulmonary secretions: positive for fungus.
Serological tests: positive for Coccidioides, Histoplasma, or Blastomyces.
Chest x-ray: typical air crescent sign surrounding the fungus ball in aspergilloma.
Aspergillus precipitins: positive in aspergilloma.
Serum total IgE and serum-specific IgE to Aspergillus fumigatus allergen: typically elevated in allergic bronchopulmonary aspergillosis and occasionally in aspergilloma.
Nocardiosis
SIGNS / SYMPTOMS
Typically occurs in immunocompromised patients with impaired cell-mediated immunity (e.g., AIDS, transplant immunosuppression, malignancies).
INVESTIGATIONS
Gram and acid-fast staining and culture of pulmonary secretions: positive for Nocardia.
Actinomycosis
SIGNS / SYMPTOMS
Manifestations of cutaneous actinomycosis with nodular lesions that tend to form fistulae may be present.
INVESTIGATIONS
Diagnosis is based on identification of characteristic sulfur granules in pus.
Gram and periodic acid-Schiff staining of histological specimens: presence of actinomycotic colonies.
Anaerobic culture of pulmonary secretions: positive for Actinomyces.
Granulomatosis with polyangiitis (Wegener's)
SIGNS / SYMPTOMS
Upper respiratory tract and renal involvement are common. Ocular, cutaneous, musculoskeletal, and neurological manifestations are usually present.
INVESTIGATIONS
Positive anti-neutrophil cytoplasmic antibody combined with positive specific proteinase 3 antibody testing by enzyme immunoassay.
Urinalysis: haematuria and proteinuria.
Rheumatoid lung nodule
SIGNS / SYMPTOMS
Symmetrical arthritis of the small joints of the hands and feet with morning stiffness are common manifestations.
INVESTIGATIONS
Chest x-ray: pulmonary nodules with cavitation usually located in the upper lobe (Caplan's syndrome).
Rheumatoid factor: positive.
Anti-cyclic citrullinated peptide antibody: positive.
Aseptic lung abscess
SIGNS / SYMPTOMS
Affects mostly patients with inflammatory bowel disease. Splenic and hepatic abscesses are often present. Lack of clinical improvement despite prolonged antibiotic treatment. Vast majority of patients respond to high-dose corticosteroids.[39]
INVESTIGATIONS
Diagnosis is made by ruling out infection in a person with radiological evidence of deep abscesses and lack of response to conventional antibiotic therapy.
Bacterial and fungal blood cultures: negative.
Serological testing for viral and bacterial aetiologies: negative.
Culture and polymerase chain reaction (PCR) of purulent material aspirated from splenic abscesses: negative.
Use of this content is subject to our disclaimer