Approach
Medicine-induced gynaecomastia is common. Anabolic steroid usage, medicines that reduce testosterone synthesis or impair testosterone action, medicines that increase oestrogen levels, hormone therapy for gender dysphoria, and prostate cancer treatment are strong risk factors for development of gynaecomastia.
Gynaecomastia can be physiological in newborns and pubertal boys. Pre-pubertal boys with breast enlargement should undergo evaluation on a case-by-case basis. Environmental exposures causing gynaecomastia can be very subtle.[47][61][62] Children are particularly vulnerable.
In overweight middle-aged and older men, gynaecomastia is often asymptomatic and is found incidentally on physical examination. Usually no additional evaluation is needed in this setting. Symptomatic men are more likely to note irritation than pain, with chafing of the breast. [Figure caption and citation for the preceding image starts]: Gynaecomastia evaluationFrom the collection of Catherine B. Niewoehner, MD [Citation ends].
History
The patient should be asked about the duration and course of symptoms. Rapid enlargement in the absence of new exposures raises concern for a hormone-secreting tumour.[27]
The history should include the following.
Medicine use: include non-prescription or medicine bought over the internet, and nutritional supplements. Many medicines are associated with gynaecomastia, but establishing a causal relationship is difficult.[23] Opportunities for children to obtain adult medicines (including contraceptives) should be reviewed.
Environmental exposure: possible endocrine-disrupting chemicals, alcohol, marijuana, heroin, and cocaine.[27][63] Workplace and other environmental exposures to oestrogens, phytoestrogens, and androgens should be considered.
Specific symptoms of hypogonadism: erectile dysfunction, decreased libido, loss of body hair, decreased strength. Any history indicating abnormal sexual development, including precocious puberty, should be elicited.
General past medical history: including possible malnutrition, should be evaluated.
Symptoms of hyperthyroidism: heat intolerance, weight loss, palpitations, tremor.
Liver impairment: such as cirrhosis (increasing abdominal girth, jaundice).
Renal insufficiency: loss of appetite, fluid retention, tiredness.
Physical examination
Includes: breast examination; assessment for being overweight; signs of hyperthyroidism, liver impairment, or renal insufficiency; and testicular examination.
Breast examination[11][16][27]
Should be done in the supine position.
Thumb and forefinger are placed on the outer and inner breast margins and are brought together in a pincer movement along the chest wall until they reach a mound of firm breast tissue located concentrically under the nipple/areola.
The diameter is measured with a ruler or measuring tape.
A diameter 2 cm or less is considered normal in an adult.
If breast enlargement is due only to adipose tissue (pseudo-gynaecomastia), resistance to palpation is felt only beneath the nipple. Gynaecomastia can be unilateral (10% to 25%) and might be tender.[8][11] Malignancy is suspected if there is a unilateral eccentric mass; any nipple, areola, or skin abnormality (such as dimpling or breast discharge); or axillary adenopathy. If the clinical picture is suspicious for a malignant lesion, biopsy may be performed (in preference to imaging).[3]
Assessment for being overweight
Body mass index (BMI) 25 to 29.9 kg/m².
BMI ≥30 kg/m² (obese).
Before 18 years of age, being overweight is defined by 85th to 95th percentiles for BMI for age and sex; for obesity it is above 95th percentile.
Signs of hyperthyroidism, liver impairment, or renal insufficiency
Tremor, goitre (hyperthyroidism).
Ascites, spider angiomata (liver impairment).
Fluid retention, sallow skin colour, tremors (renal insufficiency).
Testicular examination[39][40][41]
Assess for small size, mass, or abnormal consistency.
Marked muscle development, small firm testicles, and adult acne suggest exogenous androgen exposure.
Decreased body hair, female fat distribution, decreased strength, or small or soft testicles suggest hypogonadism.
A mass may suggest human chorionic gonadotrophin (hCG)-producing tumour or Leydig cell tumour.
Laboratory evaluation
If the cause of gynaecomastia is not obvious, measurement of thyroid-stimulating hormone, creatinine, and liver function tests should follow.
If these are normal, luteinising hormone (LH), testosterone, sex hormone binding globulin (SHBG), estradiol, beta-hCG, dehydroepiandrosterone sulphate (DHEAS), and prolactin are measured. LH and testosterone have a diurnal rhythm and should be measured in the morning when levels are highest.[27][64] Testosterone is ideally measured by a specific assay such as liquid chromatography tandem mass spectrometry.[64]
A free testosterone level, measured by equilibrium dialysis, may be helpful in assessing the bio-availability of male hormone if total testosterone is equivocal.
No laboratory abnormality is found in the majority of patients with chronic gynaecomastia found incidentally on physical examination, compared with 25% of cases with recent onset.[20][Figure caption and citation for the preceding image starts]: Hormones involved in male breast developmentFrom the collection of Catherine B. Niewoehner, MD [Citation ends].
Imaging
Breast imaging is indicated when the clinical examination is equivocal.[3][65]
Suspicious features on ultrasound may prompt mammography.[65][66]
Breast ultrasound is recommended if surgery is planned for gynaecomastia.[65]
Testicular ultrasound should be ordered in patients with sudden gynaecomastia onset (with or without a palpable testicular mass) and raised serum levels of oestrogen, or raised beta-hCG, to rule out testicular tumour.[3][27]
Abdominal CT or MRI should be performed if an adrenal adenoma or carcinoma is suspected based on elevations of DHEAS and estradiol, or clinical findings suggesting concomitant glucocorticoid and/or mineralocorticoid excess.[4]
Biopsy
Biopsy is prompted by any irregular, rubbery, hard, fixed, or eccentric (not sub-areolar) mass; overlying nipple, areola, or skin abnormality; or axillary adenopathy. These findings are suggestive of breast cancer.[3][Figure caption and citation for the preceding image starts]: Histology: breast cancer; nests of malignant ductal carcinoma invading tissue; 10X magnificationFrom Minneapolis Veterans Affairs Medical Center pathology collection [Citation ends].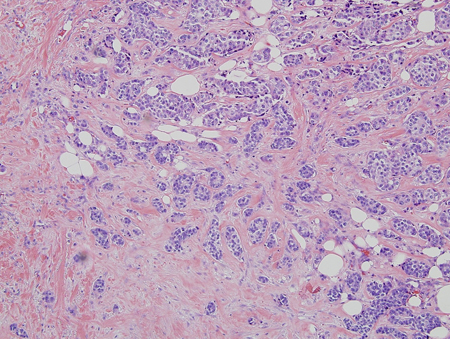
Use of this content is subject to our disclaimer