Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
secure airway + percutaneous endovascular stenting
Airway should be secured by intubation or surgically first.
Becoming increasingly used, because the stent can be placed before a tissue diagnosis is available. It is a useful procedure for patients with severe symptoms such as respiratory distress that require urgent intervention.[21][22] Meta-analyses have demonstrated that endovascular therapy with stenting has high technical and clinical success rates.[23][24][25]
Done percutaneously by obtaining access usually through the femoral vein. Performed under conscious sedation. Fluoroscopic guidance and iodinated contrast are used. Most operators use heparin during the procedure. [Figure caption and citation for the preceding image starts]: Post-dilatation of the superior vena cava stentImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].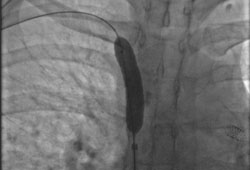 [Figure caption and citation for the preceding image starts]: Venography showing superior vena cava stenosis. Stent placement in the left pulmonary artery is seenImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Venography showing superior vena cava stenosis. Stent placement in the left pulmonary artery is seenImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Percutaneous balloon angioplasty of the stenotic lesion in superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Percutaneous balloon angioplasty of the stenotic lesion in superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Stent deployment in the superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Stent deployment in the superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].
Self-expanding or balloon-expandable stents may be used (usually bare metal stents).
Complications of percutaneous stenting are in the range of 3% to 7% and include volume overload due to sudden increase in preload, stent thrombosis, pulmonary embolus, stent migration, haematoma at the insertion site, infection, bleeding, and, very rarely, perforation or death.[22]
Patency rate is around 80% to 94%, and 20% of patients may require repeat stenting.
Bleeding risk is 1% to 14%, due to anticoagulation with aspirin, clopidogrel, and/or warfarin, which may be used following stent placement to prevent thrombosis.[21][31]
Data regarding post-procedural anticoagulation are lacking, and practices vary.[2]
percutaneous endovascular stenting
Treatment recommended for ALL patients in selected patient group
Endovascular stenting is performed to achieve more rapid improvement in symptoms and has fewer side effects compared with radiotherapy.[23][24][25]
Undertaken percutaneously by obtaining access (usually) through the femoral vein. Performed under conscious sedation. Fluoroscopic guidance and iodinated contrast are used and most operators use heparin during the procedure.[Figure caption and citation for the preceding image starts]: Post-dilatation of the superior vena cava stentImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Venography showing superior vena cava stenosis. Stent placement in the left pulmonary artery is seenImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Percutaneous balloon angioplasty of the stenotic lesion in superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].[Figure caption and citation for the preceding image starts]: Stent deployment in the superior vena cavaImage obtained from cardiac catheterisation laboratory at University of Missouri, Columbia; used with permission [Citation ends].
Self-expanding or balloon-expandable stents may be used (usually bare metal stents).
Complications of percutaneous stenting are in the range of 3% to 7% and include volume overload due to sudden increase in preload, stent thrombosis, pulmonary embolus, stent migration, haematoma at the insertion site, infection, bleeding, and, very rarely, perforation or death.[22]
Patency rate is around 80% to 94%, and 20% of patients may require repeat stenting.
Bleeding risk is 1% to 14%, due to anticoagulation with aspirin, clopidogrel, and/or warfarin, which may be used following stent placement to prevent thrombosis.[21][31]
Data regarding post-procedural anticoagulation are lacking, and practices vary.[2]
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer