Investigations
1st investigations to order
ECG for LQT1
Test
Resting ECG for LQT1.[Figure caption and citation for the preceding image starts]: ECG findings in type 1 long QT syndromeFrom the collection of Dr James P. Daubert [Citation ends].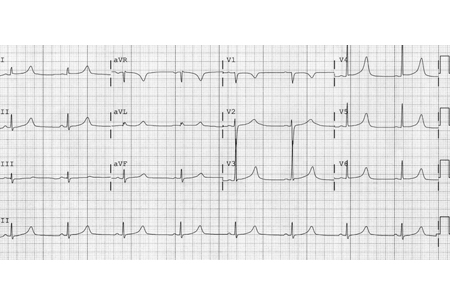
Should be undertaken in all suspected cases.[16]
QT interval and corrected QT interval (QTc) should be assessed.
T-wave morphology (monophasic or multiphasic) should be assessed.
QT interval is measured using either tangent or threshold methods.
QTc calculated using Bazett's formula: QT divided by the square root of the RR interval, where the RR interval is the interval between each QRS complex (ideally that immediately preceding the QT interval and averaged for 3 to 5 complexes).
All measurements in seconds.
Result
prolonged QT intervals associated with a broad-based T wave
ECG for LQT2
Test
Resting ECG for LQT2.[Figure caption and citation for the preceding image starts]: ECG findings in type 2 long QT syndromeFrom the collection of Dr James P. Daubert [Citation ends].
Should be undertaken in all suspected cases.[16]
QT interval and QTc should be assessed.
T-wave morphology (monophasic or multiphasic) should be assessed.
QT interval is measured using either tangent or threshold methods.
QTc calculated using Bazett's formula: QT divided by the square root of the RR interval, where the RR interval is the interval between each QRS complex (ideally that immediately preceding the QT interval and averaged for 3 to 5 complexes).
All measurements in seconds.
Result
low-amplitude and notched T waves
ECG for LQT3
Test
Resting ECG for LQT3.[Figure caption and citation for the preceding image starts]: ECG findings in type 3 long QT syndromeFrom the collection of Dr James P. Daubert [Citation ends].
Should be undertaken in all suspected cases.[16]
QT interval and QTc should be assessed.
T-wave morphology (monophasic or multiphasic) should be assessed.
QT interval is measured using either tangent or threshold methods.
QTc calculated using Bazett's formula: QT divided by the square root of the RR interval, where the RR interval is the interval between each QRS complex (ideally that immediately preceding the QT interval and averaged for 3 to 5 complexes).
All measurements in seconds.
Result
long ST segments with a late-appearing T wave resulting in a long QT interval
ECG for hypokalaemia and hypomagnesaemia
Test
Hypokalaemia is a known cause of acquired LQTS.
Should be undertaken in all suspected cases.
QT interval and QTc should be assessed.
T-wave morphology (monophasic or multiphasic) should be assessed.
QT interval is measured using either tangent or threshold methods.
QTc calculated using Bazett's formula: QT divided by the square root of the RR interval, where the RR interval is the interval between each QRS complex (ideally that immediately preceding the QT interval and averaged for 3 to 5 complexes).
All measurements in seconds.
Result
ST depression, flattened T waves, prominent U waves, and prolonged QT interval in hypokalaemia; ECG changes of co-existing hypokalaemia in hypomagnesaemia
ECG for hypocalcaemia
Test
Hypocalcaemia is a known cause of acquired LQTS.
Should be undertaken in all suspected cases.
QT interval and QTc should be assessed.
T-wave morphology (monophasic or multiphasic) should be assessed.
QT interval is measured using either tangent or threshold methods.
QTc calculated using Bazett's formula: QT divided by the square root of the RR interval, where the RR interval is the interval between each QRS complex (ideally that immediately preceding the QT interval and averaged for 3 to 5 complexes).
All measurements in seconds.
Result
isolated prolongation of the QT interval
ECG for complete atrioventricular (AV) block
Test
AV nodal block may result in QT prolongation or pause-dependent QT prolongation.
Result
sinus rhythm with normal atrial rate (represented by P-wave rate), no relationship between P waves and QRS complexes, widening of QRS complex, ventricular rate (represented by QRS complex rate) <50 bpm
serum potassium
Test
Hypokalaemia may precipitate symptoms in patients with unrecognised congenital LQTS or be the primary cause of acquired LQTS.
Result
hypokalaemia
serum magnesium
Test
Hypomagnesaemia may precipitate symptoms in patients with unrecognised congenital LQTS or be the primary cause of acquired LQTS.
Result
hypomagnesaemia
serum calcium
Test
Hypocalcaemia may precipitate symptoms in patients with unrecognised congenital LQTS or be the primary cause of acquired LQTS.
Result
hypocalcaemia
Investigations to consider
Holter monitor
Test
To evaluate the behaviour of the QT interval during bradycardia (at night), tachycardia, or sudden pauses (e.g., post-extrasystolic).
To identify non-sustained ventricular arrhythmias in asymptomatic patients with LQTS.
A Holter monitor-derived 'QT clock' may be used to improve detection of QT prolongation.[39]
Result
intermittent QT and corrected QT interval prolongation associated with ventricular arrhythmias
exercise tolerance test
Test
Especially useful in the diagnosis of LQT1.
QT and corrected QT interval increase more in LQT1 than in LQT2 and LQT3.
Useful for diagnosis when the QT interval is borderline prolonged.
Assists in the prescription of a maximum exercise level for patients presenting with exercise-induced symptoms of presyncope or syncope.
Result
QT and corrected QT interval prolongation
echocardiography
Test
To assess for and rule out regional wall motion abnormalities suggestive of myocardial scarring or infarction.
Helpful in ruling out and characterising valvular stenotic or regurgitant lesions.
Result
assessment of regional wall motion and valve function
genetic testing
Test
Pinpoints the channelopathy responsible for the LQTS, thus identifying the subtype.[41]
Aids risk stratification of patients.
Allows mapping of the mutation's inheritance so family members can be screened.
Relatively low sensitivity of approximately 70%, requires expert interpretation, and is very costly.[5][42] In the absence of a family history of LQTS, it is not indicated for asymptomatic individuals with borderline QTc intervals (<480 ms). However, genetic testing is indicated when there is a very strong clinical diagnosis or when the QTc exceeds 500 ms on serial ECGs and a reversible cause is absent.[5][42]
Patients with multiple LQTS gene mutations are at higher risk for breakthrough cardiac events during follow-up.[43]
Result
mutations in the KCNQ1 gene in LQT1, mutations in the KCNH2 gene in LQT2, mutations in the SCN5A gene in LQT3
adrenaline (epinephrine) test
Test
Must be performed with immediate access to advanced life support and external defibrillation.
Especially useful in the diagnosis of LQT1.
Result
QT and corrected QT interval prolongation
Use of this content is subject to our disclaimer