Investigations
1st investigations to order
clinical examination
Test
The diagnosis of an anorectal abscess is usually suspected from a patient's clinical history and confirmed by physical examination.
An adequate anorectal examination can usually be performed in the office or emergency department, though on occasion this may be impossible because of pain. Inter-sphincteric and supra-levator abscesses in particular require anaesthesia for full examination.
Result
often a clinical diagnosis, although occasionally examination under anaesthetic is required
examination under anaesthetic
Test
Performed when an adequate examination cannot be performed without anaesthesia.
On occasion, examination without anaesthetic may be impossible because of pain. Inter-sphincteric and supra-levator abscesses in particular may require anaesthesia for full examination.
Result
detection of presence of abscess
Investigations to consider
WBC count
Test
This may be useful in the evaluation of a patient with a suspected anorectal abscess and helps to confirm this diagnosis.
While an elevated WBC count is very sensitive, it is not specific for an anorectal abscess and the absence of leukocytosis does not exclude the diagnosis.
Result
may be elevated with increased proportion of granulocytes (left shift)
serum glucose
Test
Useful for the management of diabetic patients with a suspected anorectal abscess, though it may be difficult to treat the hyperglycaemia prior to drainage of the abscess.
Result
normal or hyperglycaemia
serum electrolytes
Test
An elevated urea and creatinine, decreased bicarbonate, and an increased base deficit (metabolic acidosis) are common findings in patients with necrotising soft-tissue infections and life-threatening sepsis associated with their anorectal abscess.
Abnormal blood chemistry results should generally be evaluated further only after the acute abscess has been treated, while addressing any urgent treatment considerations acutely (e.g., volume depletion, hyperglycaemia).
Result
usually normal; may show elevated urea and creatinine, decreased bicarbonate
anal ultrasonography
Test
Anal ultrasonography is an inexpensive means to diagnose anorectal abscesses, though it is not normally needed for diagnosis of uncomplicated cases.
Excessive discomfort with this modality also limits its use in the diagnosis of inter-sphincteric and supra-levator abscesses.[5]
Result
visualisation of anorectal abscesses
CT pelvis
Test
Considered in patients with suspected occult abscess or atypical presentation.[4][5][6] Most anorectal abscesses are easily visualised with CT.[Figure caption and citation for the preceding image starts]: CT demonstrating a perirectal abscessFrom the collection of Dr C. Neal Ellis; used with permission [Citation ends].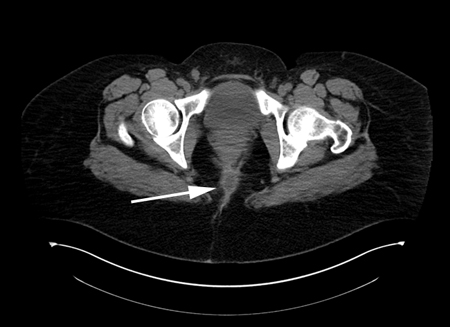
CT may be a very useful adjunct to clinical assessment in patients with severe perirectal inflammation who are difficult to examine without anaesthesia.[22]
Result
visualisation of anorectal abscesses
MRI pelvis
Test
Considered in patients with suspected occult abscess or atypical presentation.[4][5][6] Most anorectal abscesses are easily visualised with MRI. MRI is able to identify clinically occult fistula tracts as well as confirming the presence of anorectal abscess.[5]
Result
visualisation of anorectal abscesses; may reveal associated occult fistula tracts
microscopic examination and/or culture of the purulent fluid
Test
Very rarely needed or helpful except in some developing regions.
Culture of the contents of an anorectal abscess is usually reserved for patients with recurrent abscesses without a fistula identified, or for those with risk factors for one of the rare causes of anorectal abscess such as HIV or immunosuppression, or patients from a developing region. Specific microbiological and culture techniques may be needed to identify these unusual pathogens.[20][21] The contents of the abscess cavity should be stained for acid-fast bacilli and examined with a microscope to exclude tuberculosis. If actinomycosis is suspected, the fluid should be examined microscopically for sulfur granules.
Result
may be positive for infective organism; rarely positive for tuberculosis or actinomycosis
Use of this content is subject to our disclaimer