Approach
A directed history and dilated fundus examination are typically sufficient to diagnose AMD. Prognosis and treatment are dependent on the type of AMD and severity of disease. Ancillary studies may be used as indicated to differentiate type and severity of disease and to plan treatment strategies.
Clinical evaluation
Key components of the directed history are age and smoking history.
A family history of AMD may suggest a genetic predisposition.
In the early stages of the disease, patients may have no history of visual complaints or very mild distortion of vision. Other symptoms include micropsia, metamorphopsia, decreased vision, scotoma, photopsia, and difficulties with dark adaptation.[23][30]
A patient presenting with the neovascular form of the disease may report a sudden-onset distortion in the visual field of one eye.
End-stage disease may present with a history of gradual progressive loss of vision in one or both eyes.
Ophthalmic examination
Both eyes are examined for signs of disease because AMD is often bilateral. Initial and follow-up examination comprises a comprehensive eye examination, Amsler grid examination, and stereo biomicroscopic examination of the macula by slit-lamp.[23]
An Amsler grid examination of the involved eye may reveal a central area of distortion or scotoma.
Dilated fundus examination identifies characteristics of disease and determines the stage of disease.
Patients in the early stages of disease will typically have medium-sized drusen.[Figure caption and citation for the preceding image starts]: Early AMD (Age-Related Eye Disease Study Group [AREDS] category 2)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].

Patients with intermediate disease will typically have pigmentary changes, and medium and/or large drusen.[Figure caption and citation for the preceding image starts]: Intermediate AMD (Age-Related Eye Disease Study Group [AREDS] category 3)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].

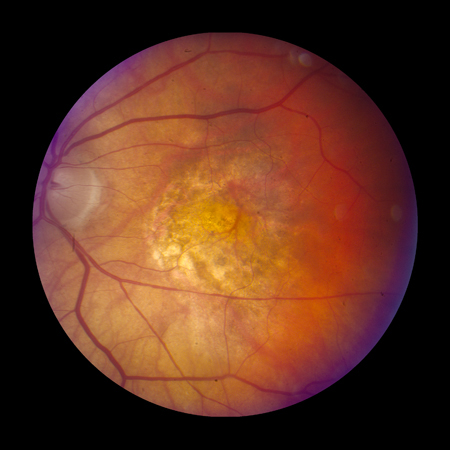
Late-stage disease is characterised by geographic atrophy and/or neovascular AMD. The signs of neovascular AMD include subretinal haemorrhage, retinal pigment epithelial detachment, retinal oedema, cysts, and lipid exudates. Long-standing neovascular disease can present with severe visual loss and a fibrovascular scar with or without subretinal fluid.[Figure caption and citation for the preceding image starts]: Late AMD with central geographic atrophy (Age-Related Eye Disease Study Group [AREDS] category 4)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Late AMD with choroidal neovascularisation with exudation (Age-Related Eye Disease Study Group [AREDS] category 4)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Late AMD with choroidal neovascularisation with exudation (Age-Related Eye Disease Study Group [AREDS] category 4)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].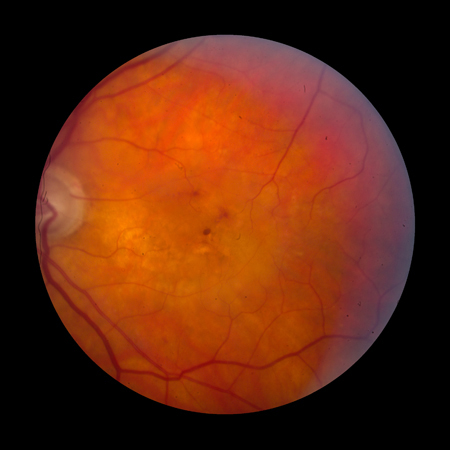 [Figure caption and citation for the preceding image starts]: Fibrovascular scar from end-stage AMD (Age-Related Eye Disease Study Group [AREDS] category 4)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Fibrovascular scar from end-stage AMD (Age-Related Eye Disease Study Group [AREDS] category 4)Reproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].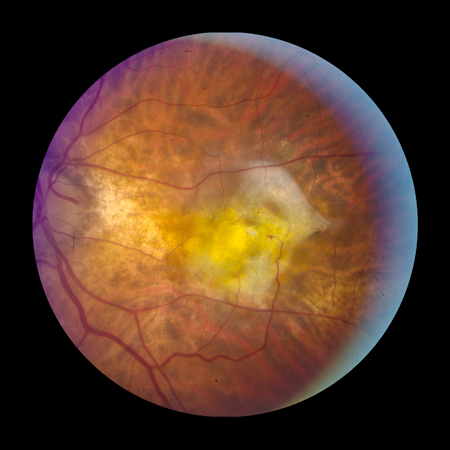
Reticular pseudodrusen are small drusen-like deposits that form between the photoreceptors and retinal pigment epithelium. The reticular form is particularly associated with progression to geographic atrophy, but pseudodrusen are also associated with progression to choroidal neovascularisation (CNV).
Imaging
Optical coherence tomography (OCT) is an important non-invasive test for diagnosing and managing AMD. It is recommended if clinical examination is suggestive of CNV.[23]
OCT can be used to:[23]
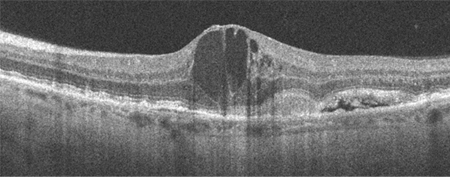
Test for or confirm the presence of subretinal or intraretinal fluid, and the degree of retinal thickening (which may not be apparent on biomicroscopy alone).
[Figure caption and citation for the preceding image starts]: High resolution optical coherence tomography image showing subretinal and intraretinal fluidReproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
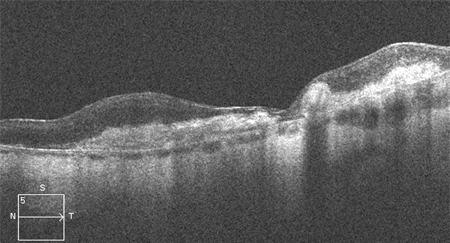
 [Figure caption and citation for the preceding image starts]: Optical coherence tomography image showing outer retinal hyper-reflective lesion, subretinal and intraretinal fluidFrom the collection of Sajjad Mahmood MA, MB BCHIR, FRCOphth; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Optical coherence tomography image showing outer retinal hyper-reflective lesion, subretinal and intraretinal fluidFrom the collection of Sajjad Mahmood MA, MB BCHIR, FRCOphth; used with permission [Citation ends].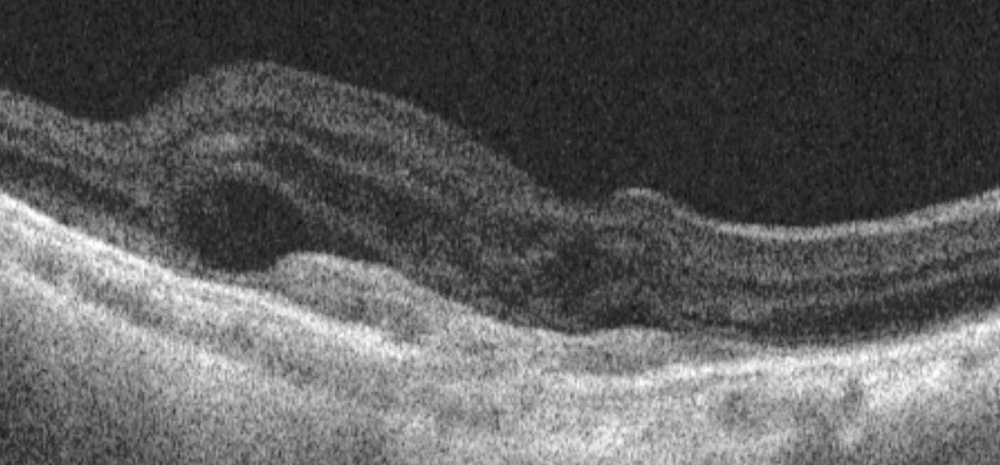
Determine the volume of intraretinal or subretinal fluid before initiating treatment for CNV
Monitor qualitative and quantitative changes in volume of subretinal and intraretinal fluid over time in response to treatment
Confirming the presence of fibrosis and a hyper-reflective (fibrovascular) scar.[Figure caption and citation for the preceding image starts]: High resolution optical coherence tomography image showing hyper-reflective scarReproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
Fluorescein angiography is the definitive test for the confirmation of CNV and may be ordered if history and/or clinical examination or OCT suggests CNV. It can be used to confirm that the blood vessels are actively leaking, as well as their anatomical location, and to measure the distance of CNV from the fovea. The result may assist in determining treatment; however, the new modality OCT angiography (described below), when available, may be preferred in the first instance, and fluorescein angiography is not needed if sufficient information is available from OCT angiography.
Fluorescein angiography can be used to rule out the presence of active CNV, unless the CNV is blocked by haemorrhage.[Figure caption and citation for the preceding image starts]: Fluorescein angiogram showing active choroidal neovascularisationReproduced from Scheie Eye Institute's patient image database; used with permission [Citation ends].
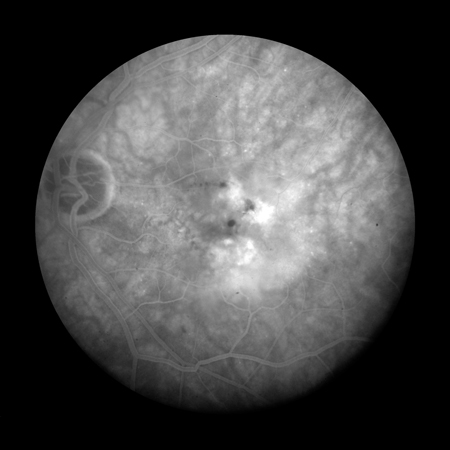
The presence of drusen (hyperfluorescence and hypofluorescence), geographic atrophy (transmission defects), and CNV (expanding hyperfluorescence) can be confirmed using fluorescein angiography.
It may assist in distinguishing classic CNV from occult CNV. Classic CNV presents with early well-defined expanding hyperfluorescence, whereas occult CNV exhibits late 'stippled' or diffuse hyperfluorescence. However, a lesion with characteristics of both types of CNV may be seen on angiography.
Indocyanine green (ICG) angiography is usually considered an adjunctive or secondary test. ICG angiography allows a better visualisation of the deeper choroidal vessels and can help identify features of idiopathic polypoidal choroidal vasculopathy, features of which may also be present in patients with neovascular AMD.[31] It can be used to detect a form of neovascularisation in AMD called retinal angiomatous proliferation. It also may be helpful in situations where the source of leakage is obscured by subretinal haemorrhage, which makes interpretation of fluorescein studies difficult.
Autofluorescence imaging is useful for delineating areas of geographic atrophy in dry AMD. It can also be used to detect reticular pseudodrusen.
OCT angiography is a technology that is becoming incorporated into OCT machines. This modality uses the change in OCT characteristics of the scanned area of retina (over time) to detect blood flow. This can be used to image blood vessels and detect CNV in only a little more time than a standard OCT scan, and without the need for intravenous administration of fluorescein. This technology is developing to overcome limitations related to artefacts. Active leak from vessels cannot be shown in the same way as fluorescein angiography, but if CNV is confirmed in conjunction with other signs of activity on the OCT scan, it may be sufficient to initiate therapy.[32][33][Figure caption and citation for the preceding image starts]: Optical coherence tomography angiography image showing hyper-reflective lesion which corresponds with a network of choroidal neovascularisation; this has proliferated in between the neurosensory retina and retinal pigment epitheliumFrom the collection of Sajjad Mahmood MA, MB BCHIR, FRCOphth; used with permission [Citation ends].
Use of this content is subject to our disclaimer