Approach
The diagnosis of jaundice is usually easy to establish based on history and observation of yellow discoloration of the sclerae, skin, and mucous membranes.[Figure caption and citation for the preceding image starts]: Jaundice: eye and skin of a patientGarry Watson/Science Photo Library [Citation ends].
History
Clinical manifestations range from completely asymptomatic to severely ill.
Ask about:
Speed of onset
Within days: usually indicates acute hepatitis caused by infection, alcohol, or drugs
Within a few weeks: more likely causes are subacute hepatitis or bile duct obstruction
Fluctuating: drug-induced, ampullary carcinoma, gallstones.
Associated symptoms
Pain: right upper quadrant pain can be particularly severe in patients with gallstones or alcoholic hepatitis. Pain related to gallstones may radiate to the right shoulder, right scapula, or around the upper abdomen. An invasive carcinoma of the head of the pancreas can cause epigastric pain radiating to the back. Most causes of hepatocellular jaundice do not cause significant pain.
Pale stools and dark urine: suggest a cholestatic cause for jaundice. Stools are coloured by stercobilinogen, which is produced by the action of intestinal bacteria on bilirubin. When the biliary tree is obstructed, bile does not enter the small intestine as usual so stercobilinogen production ceases. As a result, stools appear lighter, while urine appears darker due to increased urinary conjugated bilirubin excretion.
Anorexia, nausea and vomiting, and weight loss can occur with gallstones, malignancy, or hepatitis.
Pruritus is present in 80% to 100% of patients with cholestasis and jaundice.[76]
Fever can indicate acute hepatitis, biliary obstruction (including ascending cholangitis), leptospirosis, or amoebic liver abscess.[77]
Past medical history
Inflammatory bowel disease (increased risk of primary sclerosing cholangitis)
Inherited and acquired causes of haemolysis
Previous malignancy
History of blood transfusions before 1992. Screening of donated blood for hepatitis C started in 1992 in the US.[78] Patients who received blood before 1992 are at a higher risk of hepatitis C infection.
Any abdominal surgery.
Drug and alcohol history
All recent drugs, including prescription medication, non-prescription drugs, herbal remedies, supplements, illegal drug use (including intravenous injection). The history should cover any medication, herbal or dietary supplements taken within 180 days before presentation, due to occasional long latency intervals between ingestion and liver injury.[23]
Quantify alcohol consumption. The 10-question Alcohol Use Disorders Identification Test (AUDIT) is a simple and effective tool.[18] [ Alcohol Consumption Screening AUDIT Questionnaire Opens in new window ] A score of 8 to 15 indicates hazardous drinking, 16 to 19 indicates harmful drinking, and ≥20 indicates probable alcohol dependence. A three-question version of the test, the AUDIT-C, has been shown to be sensitive and specific in various medical settings.[79][80]
Travel history: to assess the likelihood of hepatitis A, hepatitis B, or parasitic infection.
Sexual history: sex of partner, type of intercourse, known intercourse with hepatitis B virus, hepatitis C virus, or HIV-infected partners. Men who have sex with men, and sexual partners of patients with chronic hepatitis B infection, are at higher risk of hepatitis B infection.[81]
Social history: non-sterile tattoos or body piercings, previous residence in countries with high prevalence of hepatitis B.
Family history: Wilson's disease, Gilbert's syndrome, autoimmune hepatitis.
Examination
The physical examination should focus on the liver and complications associated with cirrhosis.
It is important to distinguish jaundice from carotenaemia, a clinical condition characterised by yellow pigmentation of the skin and increased beta-carotene levels in the blood. In most cases, the condition follows prolonged and excessive consumption of carotene-rich foods, such as carrots, pumpkin, and sweet potatoes. The sclerae are always spared in carotenaemia, which readily distinguishes it from jaundice.
A careful skin examination may reveal track marks on the extremities, evidence of ecchymosis or petechiae, and, in some, the presence of spider angiomata and palmar erythema. Muscle wasting such as temporal wasting and loss of the thenar eminence may be observed.
The abdominal examination should include close inspection for collateral veins (caput medusae) and ascites. The liver and spleen should be palpated and percussed during both inspiration and expiration to checking for enlargement, pain, and nodularity. A nodular liver with decreased size suggests cirrhosis, and the presence of collateral vessels suggests portal hypertension.
Note the presence or absence of a palpable gallbladder. Courvoisier's law states that enlargement of the gallbladder with jaundice is likely to result from obstructive carcinoma rather than a stone in the common bile duct. With a common bile duct stone, the gallbladder is usually scarred from infection and does not distend.
Hepatic encephalopathy produces a spectrum of neurological and psychiatric signs. Assessment of a patient's level of consciousness, as well as physical examination findings such as asterixis, is essential. The West Haven Criteria may be used to categorise hepatic encephalopathy into grades based on severity:[82]
Grade 1: subtly impaired awareness, sleep alterations, shortened attention span, impaired addition or subtraction, heightened mood or anxiety, oriented in time and space
Grade 2: lethargy or apathy, disorientation for time, obvious personality change, inappropriate behaviour, dyspraxia, asterixis
Grade 3: somnolence to semi-stupor, responsive to vocal stimuli, marked confusion, gross disorientation (disoriented in time and space), bizarre behaviour; physical findings may include hyperreflexia, nystagmus, clonus, and rigidity
Grade 4: coma.
Lung examination may reveal evidence of pleural effusion (hepatic hydrothorax). Cardiovascular examination may suggest liver dysfunction due to congestion from right heart failure. Rectal examination may reveal evidence of gastrointestinal bleeding.
Laboratory tests
Initial laboratory testing for all patients should include the following:
Serum liver function tests with fractionation of the bilirubin (direct and indirect)
Three patterns of liver function derangement have been described: cholestatic, hepatocellular, and mixed.
The cholestatic pattern consists of predominant elevation of bilirubin, alkaline phosphatase, and gamma glutamyl transferase, and the hepatocellular pattern consists of elevations of bilirubin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT).
These patterns are non-specific and can significantly overlap (i.e., liver injury with features of both cholestatic and hepatocellular injury).
Note that ALT and AST levels may be normal in liver cirrhosis because there is insufficient healthy liver tissue to release elevated quantities of these enzymes.[1]
Serum AST/ALT ratio >2 is typical of alcoholic liver disease and occurs in about 70% of patients.[83] Reversal of the ratio, with ALT elevated more than AST, suggests concomitant viral hepatitis or non-alcoholic fatty liver disease as the cause of liver dysfunction in patients who misuse alcohol.
Prothrombin time (PT) and international normalised ratio (INR)
An increased PT and INR when coupled with a low albumin is indicative of synthetic liver dysfunction and suggestive of cirrhosis or acute liver failure.
INR is a component of the Glasgow Alcoholic Hepatitis Score (used to determine the severity and prognosis of acute alcoholic hepatitis) and the Model of End-stage Liver Disease (MELD) score (used to estimate relative disease severity and prognosis of patients awaiting liver transplantation).[68][84][85]
Increased PT and INR can be seen in cholestasis without synthetic liver dysfunction due to malabsorption of vitamin K.
Full blood count
A low platelet count is suggestive of portal hypertension leading to hypersplenism. Anaemia is a prominent feature in patients with liver disease and should be further investigated with iron studies.
Further laboratory tests to consider include:
Serum creatinine, urea and electrolytes
Acute kidney injury may occur in patients with acute liver failure, acute-on-chronic liver failure, and decompensated cirrhosis.
Hyponatraemia is common in cirrhosis.
Elevated urea, and elevated urea:creatinine ratio, may occur if there has been upper gastrointestinal bleeding.
Creatinine is a component of the MELD score.[68]
C-reactive protein and erythrocyte sedimentation rate (ESR).
Elevated in infection (e.g., ascending cholangitis, leptospirosis, amoebic liver abscess) and inflammatory conditions (e.g., acute-on-chronic liver failure, acute alcoholic hepatitis).
ESR may be elevated in autoimmune conditions (e.g., autoimmune hepatitis).
Serum paracetamol
Measured in cases of acute liver failure and suspected drug-induced liver injury.
Microbiological tests
Patients with decompensated cirrhosis or alcoholic liver disease should have a comprehensive infection screen including blood and urine cultures.[66][67][86]
Anti-hepatitis A virus immunoglobulin M (IgM), hepatitis B serology, hepatitis B viral load, anti-hepatitis C virus IgM and viral load, anti-hepatitis D antibody (in patients with hepatitis B infection), anti-hepatitis E antibody, if viral hepatitis is suspected.
Enzyme-linked immunosorbent assay (ELISA) for leptospirosis IgM, blood cultures, microscopic agglutination test, and leptospiral DNA polymerase chain reaction, if leptospirosis is suspected.
Immunological tests
Antinuclear antibody, anti-smooth muscle antibody, anti-liver-kidney microsome type 1 (anti-LKM-1) antibody, and anti-soluble liver antigen antibody, if autoimmune hepatitis is suspected.
Anti-mitochondrial antibody if primary biliary cholangitis is suspected.
Serum IgG4 if IgG4 cholangiopathy is suspected.
Suspected haemolysis
Haptoglobin, lactate dehydrogenase, reticulocyte count, peripheral blood smear, direct and indirect antiglobulin test, direct/indirect bilirubin.
Suspected Wilson's disease
Serum ceruloplasmin and urinary copper excretion.
Suspected alpha-1 antitrypsin deficiency
Serum alpha-1 antitrypsin levels.
Suspected hereditary haemochromatosis
Initial screening should include total iron, total iron binding capacity (TIBC), transferrin saturation (iron/TIBC), and ferritin.
If the transferrin saturation is elevated (>45%), further genetic testing should be considered.
Ascitic tap
Should be performed in all patients with decompensated cirrhosis.
Ascitic fluid is examined for absolute neutrophil count, Gram stain, microbiological culture, and fluid albumin.[66][67]
A fluid polymorphonuclear (PMN) leukocyte count >250 cells/mm³ is diagnostic of spontaneous bacterial peritonitis.[67]
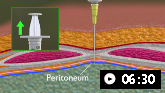 Abdominal paracentesis animated demonstration
Abdominal paracentesis animated demonstrationDemonstrates how to perform diagnostic and therapeutic abdominal paracentesis.
Chest x-ray for potential complications
Screens for pneumonia in patients with alcoholic liver disease or decompensated cirrhosis.[67]
Pleural effusions may occur as a complication of cirrhosis (hepatic hydrothorax).
Signs of heart failure (e.g., cardiomegaly, pleural effusions, pulmonary oedema) are often present in patients with congestive heart failure.[74]
Initial imaging
Most patients require some form of imaging so that mechanical obstruction can be definitively excluded and clues to hepatic and cholestatic causes identified.
For patients with jaundice who do not have predisposing conditions, ultrasound is the preferred initial modality of investigation.
Ultrasound in the diagnosis of obstructive jaundice
Obstructive processes cause dilatation of the intrahepatic or extrahepatic biliary tree, which can usually be detected using ultrasound.
Ultrasound is accurate, inexpensive, readily available, and non-invasive (with reported sensitivity of 32% to 100% and specificity of 71% to 97%) for the detection of biliary obstruction.[92] Ultrasound may indicate the location of the obstruction and whether it is likely to be benign or malignant, thus guiding the choice of subsequent imaging: computed tomography (CT) for suspected biliary or pancreatic malignancy and magnetic resonance imaging (MRI) for suspected benign causes.[92][93]
Ultrasound is limited by its decreased sensitivity for detecting biliary ductal calculi and the inability to visualise the distal common bile duct if obscured by overlying bowel gas.[92] False negatives can occur in the very early stages of obstruction before dilatation occurs.
In patients with decompensated chronic liver disease with jaundice and ascites, the addition of portal tract Doppler studies at the time of ultrasonography and subsequent triphasic CT imaging of the liver would be useful to exclude portal vein occlusion.[92]
In cases when most of the abdominal organs need to be assessed, either CT or MRI can be used, although CT more reliably displays all abdominal anatomy.[92]
Further imaging in suspected mechanical obstruction
Abdominal CT study
In patients with acute biliary obstruction and suspected complicating conditions that are not well evaluated by sonography (e.g., cholangitis, cholecystitis, or pancreatitis), a pre- and post-intravenous contrast-enhanced abdominal CT study is useful in defining the level of obstruction, likely cause, and co-existent complications.
Malignant obstruction is most commonly due to pancreatic carcinoma, but may be secondary to cholangiocarcinoma of either the proximal or distal duct or extrinsic compression of the duct by enlarged peri-ductal lymph nodes. A contrast-enhanced multipass CT examination has high sensitivity for lesion detection and 70% accuracy in discriminating resectable and unresectable disease.
CT can detect partially calcified biliary calculi, but is relatively insensitive for detecting bilirubinate or cholesterol calculi.[92]
MR studies
For detection of ductal calculi, MRI is more sensitive than CT or ultrasound.
For diagnosis of common bile duct stones, MR cholangiopancreatography has a reported sensitivity ranging from 77% to 88%, a specificity between 50% to 72%, accuracy of 83%, positive predictive value between 87% to 90%, and negative predictive value between 27% to 72%, as compared with the gold standard of endoscopic retrograde cholangiopancreatography.[92][94][95]
Endoscopic ultrasound and endoscopic retrograde cholangiopancreatography (ERCP)
In cases where CT/MRI and sonography are equivocal, ERCP and endoscopic ultrasound imaging may be of benefit allowing a cytological diagnosis to be made using fine-needle aspiration or brushing. ERCP involves passing an endoscope into the duodenum, cannulating the ampulla, and injecting contrast into the common bile duct. Fluoroscopic images of the biliary tree are obtained.
Fluorodeoxyglucose-positron emission tomography/CT may be considered in patients with obstructive jaundice and suspected pancreatic cancer not confirmed by CT.[96]
Endoscopic ultrasound or ERCP may be carried out if strictures have been identified.[39][97] For extrahepatic strictures, endoscopic ultrasound-guided tissue acquisition may be preferred over ERCP.[98]
When there is persistent clinical suspicion, but insufficient evidence of stones on abdominal ultrasonography, endoscopic ultrasonography may be used to diagnose common bile duct stones.[99]
ERCP is nearly always performed as a therapeutic procedure following confirmation of common bile duct stones or a malignant obstruction on CT or MRI imaging. A balloon sweep of the common bile duct can remove stones in 80% to 95% of cases. Sphincterotomy, stent deployment, and biopsy can also be performed. The procedure carries a 4.0% to 5.2% risk of major complications such as haemorrhage, perforation, pancreatitis, or cholangitis.[92]
Use of this content is subject to our disclaimer