Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
stretching
Treatment recommended for ALL patients in selected patient group
Tight hamstrings and equinus are common in patients with plantar fasciitis and treatment of equinus is important for all stages of the condition.[3] Stretching is aimed at the tendoachilles and the plantar fascia. It is recommended 3 times daily with 10 repetitions of each stretch.[40] Patients may be referred to a physiotherapist or podiatrist for help with technique, although formal physiotherapy has not been shown to be more effective than home stretching exercises.[41] A study found non-weight-bearing stretching exercises, specific to the plantar fascia, to be superior to the standard weight-bearing achilles tendon-stretching exercises in patients with recalcitrant pain.[42] Recommendations for stretching are based on the hypothesis that nocturnal contracture of the gastrocnemius-soleus complex contributes to the irritation of the plantar fascia and persistence of symptoms.[43][44][Figure caption and citation for the preceding image starts]: Calf stretchFrom the collection of Alex Koleszar, Cleveland Clinic; used with permission [Citation ends].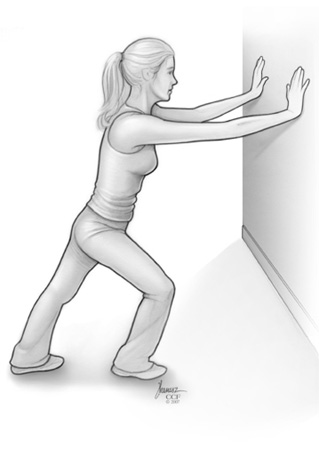 [Figure caption and citation for the preceding image starts]: Achilles stretchFrom the collection of Alex Koleszar, Cleveland Clinic; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Achilles stretchFrom the collection of Alex Koleszar, Cleveland Clinic; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Plantar stretchFrom the collection of Alex Koleszar, Cleveland Clinic; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Plantar stretchFrom the collection of Alex Koleszar, Cleveland Clinic; used with permission [Citation ends].
corticosteroid injection
Additional treatment recommended for SOME patients in selected patient group
Corticosteroid injections are used in the short term for acute pain management of plantar fasciitis. They are considered if conservative treatment leads to inadequate relief of pain, or if pain is especially high on initial presentation.
They have been shown to be efficacious in relieving pain; however, most studies report only short-term (up to 6 weeks), and not sustained, benefits.[53][54][55]
[ ![]() ]
One study, however, found that the significant reduction in thickness of plantar fascia seen at 1 month following corticosteroid injection persisted on re-scanning at 6 months.[56] A Cochrane review pooled data from 8 trials and found only a modest short-term (<1 month) benefit of glucocorticoid injections compared with placebo.[55] Another systematic review found that corticosteroid injection was more effective than some comparators (autologous blood injection, foot orthoses, and physiotherapy) for the reduction of pain and the improvement of function in people with plantar heel pain in the short term. However, it was no more effective than placebo injection for reducing pain in the short and medium term.[57]
]
One study, however, found that the significant reduction in thickness of plantar fascia seen at 1 month following corticosteroid injection persisted on re-scanning at 6 months.[56] A Cochrane review pooled data from 8 trials and found only a modest short-term (<1 month) benefit of glucocorticoid injections compared with placebo.[55] Another systematic review found that corticosteroid injection was more effective than some comparators (autologous blood injection, foot orthoses, and physiotherapy) for the reduction of pain and the improvement of function in people with plantar heel pain in the short term. However, it was no more effective than placebo injection for reducing pain in the short and medium term.[57]
Administered using a plantar medial approach, typically in combination with local anaesthetic to work as an immediate analgesic and anti-inflammatory agent. Lidocaine and bupivacaine are used in combination to achieve a faster onset and longer relief.
Complications are uncommon, but include infection, subcutaneous fat atrophy, skin pigmentation changes, fascial rupture, peripheral nerve injury, and muscle damage.[58][59]
Corticosteroid injections have shown decreased thickness of plantar fascia on sonography.
Injection therapy can be painful.[60] Post-injection pain can last for several days.
Long-lasting effects have been reported with 6-month post-procedure ultrasonography follow-up.[56] If the initial treatment was beneficial but symptoms return, the treatment may be repeated once with a minimum of 6 weeks between injections.
Primary options
bupivacaine: (0.5%) 1 mL intrafascially
and
lidocaine: (1%) 1 mL intrafascially
-- AND --
dexamethasone sodium phosphate: 4 mg intrafascially as a single dose
or
triamcinolone acetonide: 10 mg intrafascially as a single dose
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer