Investigations
1st investigations to order
FBC
Test
Performed to evaluate for evidence of infection.
A significantly elevated WBC, especially if accompanied by abdominal tenderness or peritoneal signs, is a sign that a more severe condition (e.g., sepsis, peritonitis) is present.
Result
normal or slightly elevated WBC
serum electrolytes
Test
Performed to evaluate severity and to guide supportive treatment.
A non-specific test.
Check electrolytes daily, including phosphate, in patients on parenteral nutrition to identify any electrolyte abnormalities associated with postoperative intravenous feeding and the nil by mouth state.
Result
hypokalaemia, hypo-chloraemia, alkalosis
serum magnesium
Test
Electrolyte imbalance, particularly hyper-magnesaemia, has been associated with ileus.[59]
Result
hyper-magnesaemia may be present
urea and creatinine
Test
Elevated urea and creatinine may be present in dehydrated patients.
Result
elevated blood urea and serum creatinine may occur with dehydration
arterial blood gases
Test
To evaluate for the presence of acid base disturbance.
Result
alkalosis may present in dehydrated patients; acidosis may be present in intestinal ischaemia
abdomen and pelvis CT scan (with intravenous contrast and oral water-soluble contrast)
Test
Check the patient’s kidney function, as acute kidney injury may be a contraindication to a CT scan using a contrast agent.[58]
CT scan using oral water-soluble contrast and intravenous contrast is the method of choice in differentiating prolonged ileus and mechanical obstruction.[54][56][57]
In ileus, the CT scan shows distention of the stomach, fluid filled intestines, and no evidence of a transition zone between dilated and collapsed bowel (a key indicator of obstruction). It is important to distinguish between small bowel obstruction and ileus; small bowel obstruction may progress to a more serious condition with bowel ischaemia if there is a twist of the intestines or vascular compromise.
In postoperative patients, a CT scan should be performed if the presumed ileus has not resolved in 3 to 4 days, or if the clinical condition of the patient worsens.
[Figure caption and citation for the preceding image starts]: CT scan with intravenous and oral contrast showing fluid-filled small intestine and caecum in ileus [Citation ends].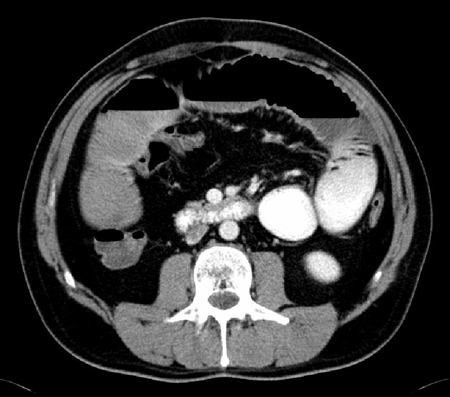 [Figure caption and citation for the preceding image starts]: CT scan with intravenous and oral contrast showing fluid-filled small intestine in ileus [Citation ends].
[Figure caption and citation for the preceding image starts]: CT scan with intravenous and oral contrast showing fluid-filled small intestine in ileus [Citation ends].
Practical tip
In general, do not use plain radiography of the chest and abdomen to differentiate prolonged ileus and mechanical obstruction.
Result
fluid filled intestines; distended stomach; no evidence of a transition zone between dilated and collapsed bowel (a key indicator of obstruction)
Investigations to consider
serum LFTs
Test
To exclude other conditions that may contribute to ileus, such as cholecystitis or pancreatitis.
Result
normal in ileus
serum lipase or amylase
Test
Use serum lipase testing (if available) in preference to serum amylase.[60]
Serum lipase and amylase have similar sensitivity and specificity but lipase levels remain elevated for longer (up to 14 days after symptom onset vs. 5 days for amylase), providing a higher likelihood of picking up a diagnosis of pancreatitis in patients with a delayed presentation.[61]
Acute pancreatitis is an important differential diagnosis for a patient presenting with acute, severe abdominal pain.
Result
normal in ileus; a result >3 times the upper limit of the normal range confirms the diagnosis of acute pancreatitis in a patient with acute upper abdominal pain
small bowel series with oral water-soluble contrast
Test
In cases of prolonged ileus (lasting 4 days or longer post-surgery), a small bowel series using oral water-soluble contrast may be done to evaluate for any evidence of mechanical obstruction that may have been missed on CT scan.
Care should be taken, as there is a risk of aspiration.
[Figure caption and citation for the preceding image starts]: Small bowel series showing dilated small bowel loops in ileus; nasogastric tube is seen curled in the stomach [Citation ends]. [Figure caption and citation for the preceding image starts]: Small bowel series showing dilated contrast-filled small bowel loops in ileus; some contrast is visible in the right colon [Citation ends].
[Figure caption and citation for the preceding image starts]: Small bowel series showing dilated contrast-filled small bowel loops in ileus; some contrast is visible in the right colon [Citation ends].
Result
no evidence of obstruction or bowel leak
gastric emptying study
Test
Consider performing this test in cases of prolonged ileus, especially in patients with comorbidities such as long-standing diabetes mellitus, which is associated with gastroparesis.
Result
delayed gastric emptying
Use of this content is subject to our disclaimer