Complications
Chronic hyponatraemia, if left untreated, can contribute to altered mentation, abnormal gait, osteoporosis, falls, and increased risk of significant fractures. Outpatient maintenance of SIADH-related hyponatraemia is of utmost importance to avoid associated increased morbidity and mortality.
Occurs in people with longstanding SIADH who undergo overaggressive treatment of hyponatraemia.[35]
The brain adapts slowly to hyponatraemia by secretion of intracellular solutes such as sodium and potassium initially, followed by amino acids and myoinositol (organic osmolytes).
Overcorrection of hyponatraemia can subject solute-poor cerebral cells to shrinkage and CPM.
CPM is characterised by demyelination of pontine, basal ganglion, and cerebellar regions with resultant neurological symptoms, including behaviour disturbances, lethargy, dysarthria, dysphagia, paraparesis or quadriparesis, and coma.[Figure caption and citation for the preceding image starts]: Pontine demyelination in axial T2 MRI sequencesFrom: P. J. Serrano-Castro, G. Alonso-Verdegay, G. López-Martínez, et al. BMJ Case Reports 2009; doi:10.1136 [Citation ends].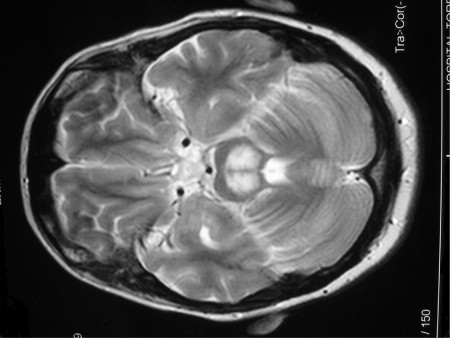
Seizures may also be seen, but are less common.[22]
One case study of patients with hyponatraemic encephalopathy, reported in early 2015, included 71 hyponatraemic episodes in which patients were treated with aggressive 3% NaCl resuscitation.[36] Twelve of the patients in the study died of comorbid conditions prior to 6-month follow-up. Of those who were re-evaluated, no patient demonstrated neurological symptoms consistent with cerebral demyelination.
Malnutrition, potassium depletion, and hepatic failure increase the risk of developing CPM.[22][23]
CPM occurs more frequently in long-standing SIADH, due to brain adaptation to hyponatraemia. It can also occur in acute SIADH (duration ≤48 hours), but this is less likely.
To treat overcorrection of hyponatraemia (either as a result of aggressive salt administration or of spontaneous water diuresis after offending medicines are discontinued), free water is replenished through increased oral intake or hypotonic fluids.
Use of this content is subject to our disclaimer