Aetiology
The molecular basis of the disorder is the absence of a functionally active multi-drug resistance-associated protein called MRP2, also known as human canalicular multi-specific organic anion transporter gene (cMOAT). MRP2 is encoded by a single-copy gene located on chromosome 10q24. Mutations of this gene have been shown to produce a highly defective MRP2 that is associated with DJS.[19][20][21] It is inherited in an autosomal recessive manner.
Pathophysiology
The primary defect in DJS is impaired transport of glucuronides and other anionic conjugates from the hepatocytes into bile, due to mutation of multi-drug resistance-associated protein 2 (MRP2). MRP2 is an integral membrane glycoprotein expressed mainly in the canalicular (apical) membrane of hepatocytes where it functions as an ATP-dependent export pump for endogenous and exogenous anionic conjugates.
The conjugated hyperbilirubinaemia seen in DJS results from defective transport of bilirubin glucuronide across the membrane that separates the hepatocyte from the bile canaliculi. Deficient excretion of bilirubin glucuronides at the canalicular membrane in the presence of otherwise normal intrahepatic metabolism results in reflux of conjugated bilirubin back into the circulation.[22][23]
MRP2 also plays an important role in the detoxification of many drugs by transporting a wide variety of compounds, especially conjugates of glutathione, glucuronate, and sulphate.
In addition to hepatocytes, MRP2 is located in renal proximal tubular cells, enterocytes, and syncytiotrophoblasts of the placenta.[22][24]
A striking characteristic of DJS is the brown to black discoloration of the liver. There is still debate as to the nature of this pigment, which is located in the lysosomes. Although originally thought to be lipofuscin, more recent data provide conflicting evidence for a relationship to melanin or polymerised epinephrine or other metabolites that accumulate in the lysosomes. It is hypothesised that these pigments accumulate in the liver because of impaired secretion of various metabolites from the hepatocyte into the bile. This pigment disappears from the liver during acute viral hepatitis, with subsequent reappearance.[6][25][26][27][28][Figure caption and citation for the preceding image starts]: Masson-Fontana stain showing the pigment in a patient with DJSPersonal collection of Professor Bernard Portmann, King's College Hospital, London, with permission [Citation ends].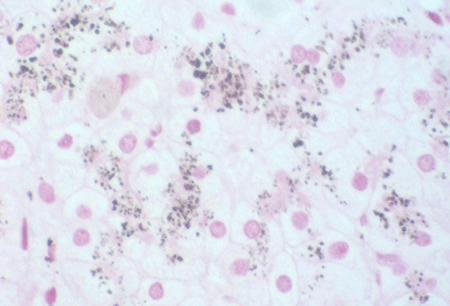
Use of this content is subject to our disclaimer