Criteria
International classification of radiographs for pneumoconiosis
Chest x-rays are classified and scored according to the International Classification of Radiographs of Pneumoconioses developed by the International Labour Organization (ILO).[44] In the US, regulations for coal workers' pneumoconiosis and silicosis require this classification system be used for medical screening and assessment. The assessing physician must have passed a test on classifying radiographs, administered by the National Institute for Occupational Safety and Health (NIOSH), and must be retested every 5 years.[45]
1. Technical quality of radiographs:
Good
Acceptable, with no technical defect likely to impair classification
Acceptable, with some technical defects but still adequate for classification
Unacceptable for classification
2. Assessment of parenchymal abnormalities.
Small parenchymal abnormalities (longest dimension ≤10 mm) are described by profusion, affected zones of the lung, shape (rounded or irregular) and size.
Profusion:
Refers to the concentration of small opacities in affected lung zones
Categories: 0, 1, 2, and 3
Always appear with a subcategory as 0/-, 0/0, 0/1; 1/0, 1/1, 1/2; 2/1, 2/2, 2/3; 3/2, 3/3, or 3/+
Affected zones:
Each lung field is divided into three zones (upper, middle, lower)
If there is a marked difference in profusion between zones, only those showing the greatest degree of profusion are used to classify overall profusion
Shape and size:
Rounded small opacities (diameter):
p: up to 1.5 mm
q: 1.5 to 3.0 mm
r: 3.0 to 10.0 mm
Irregular small opacities (width):
s: up to 1.5 mm
t: 1.5 to 3.0 mm
u: 3.0 to 10.0 mm
Large parenchymal opacities (longest dimension >10 mm) are described as one of three categories:
Category A: One large opacity with longest dimension up to 50 mm, or several large opacities with the sum of their longest dimensions up to 50 mm
Category B: One large opacity with longest dimension >50 mm, but not exceeding the equivalent area of the right upper zone; or several large opacities with the sum of their longest dimensions >50 mm, but not exceeding the equivalent area of the right upper zone
Category C: One large opacity with the longest dimension exceeding the equivalent area of the right upper zone, or several large opacities that when combined exceed the equivalent area of the right upper zone
3. Assessment of pleural abnormalities
Pleural plaques (localised pleural thickening)
Recorded as absent or present
Site, calcification, and extent of pleural plaques are recorded for all sites, and separately for the right and left lungs
Costophrenic angle obliteration
Recorded as absent or present, separately for the right and left lungs
Obliteration may occur without diffuse pleural thickening
Diffuse pleural thickening
Recorded as absent or present along the chest wall
In-profile or face-on, and extent recorded separately for the right and left lungs
Pleural thickening at the apex of the lung only is not generally recorded as pleural thickening
Patients with silicosis and coal workers' pneumoconiosis may have rounded opacities on chest x-ray. With progression to advanced disease, there is a conglomeration of smaller nodules to form large opacities that may cover the whole upper lobe. An individual with mild simple silicosis or coal workers' pneumoconiosis will typically have q or r opacities, with category 1 or 2 profusion. With more advanced disease, the profusion will be category 3. With even more severe disease (progressive massive fibrosis), there will be large opacities A, B, or C.
Patients with chronic beryllium disease may have irregular small opacities on chest x-ray. An individual with mild disease will typically have s or t opacities with category 1 profusion. With more advanced disease, the profusion will be category 2 or 3.
Pleural changes are seen on x-ray with asbestos exposure and not with any of these 3 types of pneumoconiosis.[Figure caption and citation for the preceding image starts]: CXR showing changes consistent with simple silicosis or coal workers' pneumoconiosisFrom the personal collection of Kenneth D. Rosenman, Michigan State University [Citation ends].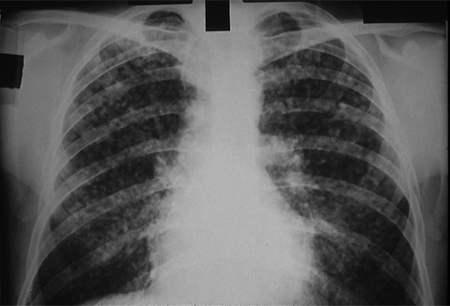 [Figure caption and citation for the preceding image starts]: CXR of chronic beryllium diseaseFrom the personal collection of Kenneth D. Rosenman, Michigan State University [Citation ends].
[Figure caption and citation for the preceding image starts]: CXR of chronic beryllium diseaseFrom the personal collection of Kenneth D. Rosenman, Michigan State University [Citation ends]. [Figure caption and citation for the preceding image starts]: CXR of progressive massive fibrosis due to silica or coal exposureFrom the personal collection of Kenneth D. Rosenman, Michigan State University [Citation ends].
[Figure caption and citation for the preceding image starts]: CXR of progressive massive fibrosis due to silica or coal exposureFrom the personal collection of Kenneth D. Rosenman, Michigan State University [Citation ends].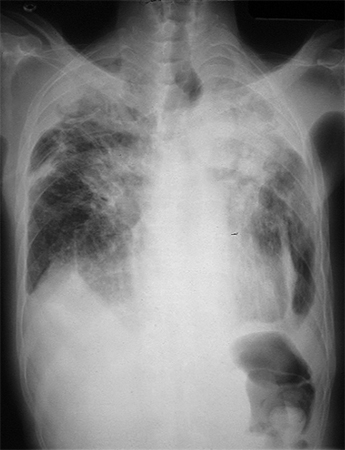
Use of this content is subject to our disclaimer