Recommendations
Urgent
Time is brain” - if you suspect a stroke, work rapidly through the initial assessment and aim for quick access to computed tomography (CT) scan.
Early initiation of reperfusion strategies (intravenous thrombolysis or mechanical thrombectomy) within 4.5 hours of onset of symptoms, if not contraindicated, is associated with improved functional outcomes.[63][64][65]
Suspect stroke in a patient with sudden (new, acute onset, or on awakening from sleep) focal neurological symptoms:[66]
Unilateral weakness or paralysis in the face, arm, or leg
Unilateral sensory loss
Dysarthria or expressive or receptive dysphasia
Vision problems (e.g., hemianopia)
Headache (sudden severe and unusual headache)
Difficulty with coordination and gait
Vertigo or loss of balance, especially with the above signs.
Exclude hypoglycaemia (a stroke mimic) as the cause of these symptoms.[67]
Use a validated tool to aid diagnosis in people with suspected stroke:[67]
In the emergency department: use the ROSIER scale (Recognition of Stroke in the Emergency Room) to establish the diagnosis rapidly.[67]
In the community: use FAST (Face Arm Speech Test) to screen people with sudden onset of neurological symptoms for stroke.[67]
Admit everyone with suspected stroke directly to a hyperacute (or acute) stroke unit as soon as possible; UK guidelines recommend doing this within 4 hours of presentation.[67]
Determine the time of symptom onset because this is the main factor that will determine eligibility for thrombolysis (i.e., within 4.5 hours of onset for intravenous thrombolysis).[67][68]
If the onset was unwitnessed, the definition of symptom onset is the time when the patient was last seen well.[67]
Request brain imaging as soon as possible (at most within 1 hour of arrival at hospital).[68] Non-enhanced CT head is the investigation of choice in acute stroke.
Remember:
Ischaemic stroke is a clinical diagnosis based on signs and symptoms.
A normal CT scan does not rule out a stroke; particularly in the first few hours, the CT scan can be normal, or show very subtle changes of ischaemia.
Key Recommendations
Obtain a brief history (including from witnesses or next of kin) followed by an abbreviated neurological examination using the National Institutes of Health Stroke Scale.[69] [ NIH Stroke Score Opens in new window ]
This tool measures the degree of neurological deficit. Higher scores indicate a more severe stroke.
Assess the patient’s level of consciousness using the Glasgow Coma Scale. [ Glasgow Coma Scale Opens in new window ]
In people with an altered level of consciousness or coma, exclude haemorrhage and other mimics such as seizures. See Differentials.
Request brain imaging as soon as possible (at most within 1 hour of arrival at hospital).[68] CT head is the investigation of choice in acute stroke.
Consider diffusion-weighted magnetic resonance imaging (MRI) of the head with stroke-specific sequences (diffusion-weighted imaging [DWI] with susceptibility weighted imaging [SWI] or T2*-weighted imaging) if the diagnosis remains uncertain despite radiology.[68]
Patients with stroke with a delayed presentation for whom reperfusion (thrombolysis or mechanical thrombectomy) is potentially indicated should have CT or MR perfusion as soon as possible (at most within 1 hour of arrival at hospital). An alternative for patients who wake up with stroke is MRI measuring DWI-FLAIR mismatch (diffusion-weighted MRI and fluid-attenuated inversion recovery MRI mismatch).[68]
In patients with a suspected large vessel occlusion who are candidates for endovascular thrombectomy, request CT angiography after the initial brain scan.[68]
Candidates for thrombectomy alone include patients who cannot receive thrombolysis (e.g., with contraindications including recent surgery or current anticoagulation use).[68]
In candidates for thrombectomy in addition to thrombolysis, request CTA or MRA with contrast after (or with) the initial CT head.[67]
Do not delay therapy with intravenous thrombolysis (if indicated) while:
Waiting for results or waiting to perform tests, unless you suspect contraindications that must be ruled out first (eg., hypoglycaemia, coagulopathy).[70][71] Treatment should be started within 4.5 hours of onset of stroke symptoms AND after excluding intracranial haemorrhage.[67][68]
Waiting to perform CTA or MRA, or waiting for results.[70]
Order in all patients:
Serum glucose to exclude hypoglycaemia and hyperglycaemia before giving thrombolysis.[67][69]
Serum electrolytes to exclude electrolyte disturbance as a cause for sudden onset of neurological signs.
Serum urea and creatinine to exclude renal failure because it may be a potential contraindication to some stroke interventions.
Cardiac enzymes to exclude concomitant myocardial infarction.
Full blood count to exclude anaemia or thrombocytopenia prior to possible initiation of thrombolysis, anticoagulants, or antithrombotics.
Prothrombin time and partial thromboplastin time (with international normalised ratio) to exclude coagulopathy.
ECG to exclude cardiac arrhythmia or ischaemia, which are relatively common in ischaemic stroke.
Consider a serum toxicology screen if you suspect ingestion of toxic substances. Signs and symptoms may mimic stroke.
Suspect stroke in a patient with sudden (new, acute onset, or on awakening from sleep) focal neurological symptoms:[66]
Unilateral weakness or paralysis in the face, arm, or leg
Unilateral sensory loss
Dysarthria or expressive or receptive dysphasia
Vision problems (e.g., hemianopia)
Headache (sudden severe and unusual headache)
Difficulty with coordination and gait
Vertigo or loss of balance, especially with the above signs.
Be aware that one or more transient ischaemic attacks (TIAs), which may be stereotypical, might precede a stroke (as warning signs or symptoms).
A TIA is a medical emergency heralding a significant risk of stroke. TIAs typically last a matter of minutes. They should be treated and investigated promptly. UK guidelines recommend that people who have had a suspected TIA (without risk stratification) should have specialist assessment and investigation within 24 hours of symptom onset.[67][68] Patients with suspected TIA should be given aspirin 300 mg immediately, unless contraindicated.[68] See Transient ischaemic attack.
Initial assessment
The goal of the initial assessment is to recognise a stroke quickly - “time is brain.
Efficient, rapid initial assessment and rapid access to CT scan (at most within 1 hour of presentation) allow for early initiation of reperfusion (intravenous thrombolysis or mechanical thrombectomy) within 4.5 hours of onset of symptoms, if not contraindicated, which is associated with improved functional outcomes.[63][64]
In the emergency department
Use the ROSIER scale (Recognition of Stroke in the Emergency Room) in those with suspected stroke or TIA to establish the diagnosis rapidly.[67][72]
Score -1 point for each feature (clinical history):
Loss of consciousness or syncope
Seizure activity
Score +1 point for each feature (neurological history):
Asymmetrical face weakness
Asymmetrical arm weakness
Asymmetrical leg weakness
Speech disturbance
Visual field defect
A score >0: stroke likely; a score ≤0: stroke unlikely (but not excluded).
In the community
Use a validated tool such as FAST (Face Arm Speech Test) to screen people with sudden onset of neurological symptoms (such as visual disturbance or balance problems) for a diagnosis of stroke:[67][73]
Score 1 point for each feature:
Face weakness
Arm (or leg) weakness
Speech disturbance
Suspect stroke if score >0; refer for emergency medical care in hospital (by 999 ambulance in the UK).
Practical tip
Be aware that the patient may have ongoing focal neurological deficits despite a negative FAST. Continue to manage them as you would someone with acute stroke.[68]
Evidence: FAST and ROSIER scales to identify stroke
Despite very limited evidence, guidelines recommend using validated screening tools to expedite access to specialist care for patients with stroke or TIA in the pre-hospital setting. There are fewer guideline recommendations on the use of these tools in the emergency department (ED) setting.[67][68][74]
[ ![]() ]
]
Pre-hospital setting
The 2023 National Clinical Guideline for Stroke for the UK and Ireland recommends the Face Arms Speech Time (FAST) test in the pre-hospital phase, but states that further evidence is required before Recognition of Stroke in the Emergency Room (ROSIER) can be recommended to screen for non-FAST symptoms in the pre-hospital phase.[68]
The recommendation for use of FAST is based on working party consensus and the results of a single diagnostic accuracy study comparing ambulance paramedics using FAST versus primary care doctor versus ED referrals for 487 people with suspected stroke to a stroke unit.[73]
The study found ambulance paramedics’ stroke diagnosis using FAST gave a positive predictive value (PPV; i.e., the proportion with a positive test who in reality actually have the condition or characteristic) of 78% (95% CI 72% to 84%).[73]
FAST may not identify some people with symptoms of stroke (e.g., sudden-onset visual disturbance, lateralising cerebellar dysfunction).
Community-based clinicians should continue to treat a person as having a suspected stroke if they are suspicious of the diagnosis despite a negative FAST test.
The UK National Institute for Health and Care Excellence (NICE) stroke guideline from 2008 (not changed in the 2022 update) also recommends using a validated tool, such as FAST, outside hospital, citing evidence from the same diagnostic accuracy study.[67][73]
A 2017 European Academy of Neurology and European Stroke Organisation consensus statement for pre-hospital management of stroke makes no recommendation for a specific scale, but instead states:
To use a simple pre-hospital stroke scale (no specific one recommended), despite the lack of evidence. In their view, benefit would outweigh possible harm and minimal resource use.
To be aware that the scales (currently available at the time of this guidance) are not sensitive enough to detect posterior circulation stroke.
Emergency department setting
NICE recommends using a validated tool, such as ROSIER, in the emergency department.[67]
This recommendation is underpinned by a validation study for the ROSIER tool, including 343 patients with suspected stroke in the ED in the development phase and 173 in the validation phase.[72]
In this study, ROSIER showed a PPV of 90% (95% CI 85% to 95%) when used by ED clinicians.[72]
The National Clinical Guideline for Stroke for the UK and Ireland makes no specific recommendation on the use of ROSIER to screen for stroke in the hospital ED setting.[68]
Symptoms/signs according to the location of infarct
Anterior circulation stroke
Associated with ischaemia related to occlusion of the anterior circulation arteries - the carotid territory, including the anterior and middle cerebral arteries and their branches.[75] Anterior circulation strokes are the most common of all ischaemic strokes.[76]
Look for one or more of the following symptoms/signs:[75]
Limb and/or facial weakness
Complete or partial loss of muscle strength in face, arm, and/or leg; a typical presentation of stroke.
Weakness in face, arms, and legs (all three at same time) suggests deep hemispheric involvement, although this may not differentiate stroke mechanism.
Expressive and/or receptive dysphasia
Sensory loss (numbness) in face and upper and/or lower extremities
Patients often describe sensory loss and paraesthesias as “numbness”.
Unilateral sensory loss on neurological examination may involve some or all primary modalities.
Cortical sensory loss usually impairs fine sensory processing abilities such as two-point discrimination, graphaesthesia, or stereognosis.
Vision loss in one eye or visual field deficit
Monocular vision loss may occur and is often transient.[77] This is a common early warning signal for cervical carotid stenosis. It can present as amaurosis fugax or retinal stroke (branch or central retinal artery occlusion); recognise and investigate with the same urgency. See Carotid artery stenosis.
Gaze paresis (often horizontal and unidirectional): in stroke, the eyes will look at the affected side of the brain
Consider seizure in people with wrong-way eye deviation (i.e., gaze deviation away from the side of the brain lesion, towards the hemiparetic side).
Visuospatial disturbances/neglect
Homonymous quadrantanopia.
Practical tip
Coma is unusual; it is more common in people with brain stem ischaemia.
Posterior circulation stroke
Associated with ischaemia related to occlusion of the posterior circulation arteries - the vertebral arteries in the neck, the intracranial vertebral, basilar, and posterior cerebral arteries, and their branches.[75]
Look for one or more of the following symptoms/signs:[75]
Double vision
Motor and/or sensory deficits
Motor deficits: weakness, clumsiness, or paralysis of any combination of arms and legs, up to quadriplegia, sometimes changing from one side to another in different attacks.
Sensory deficits: numbness, including loss of sensation or paraesthesia in any combination of extremities, sometimes including all four limbs or both sides of the face or mouth.
Vertigo, with or without nausea and vomiting
Typically reported as a spinning sensation; may also be described as feeling like being “on a ship in choppy seas”.
It is often associated with nystagmus.
Ataxia or disequilibrium
Dysarthria
Dysphagia
Specific cranial nerve deficits (eg., unilateral tongue weakness, diplopia)
Horner's syndrome (hemilateral triad of miosis, ptosis, and facial anhidrosis)
Homonymous hemianopia (ie., visual field loss on the left or right side of the vertical midline on the same side of both eyes)
‘Crossed’ syndromes:
Ipsilateral cranial nerves signs
Contralateral long motor or sensory tract dysfunction
Altered level of consciousness and coma.
Practical tip
Posterior circulation stroke remains more difficult to recognise and treat effectively than other types of stroke. Taking a careful history will help to identify patients with posterior circulation stroke, who may present with recurrent, stuttering, or progressive symptoms, which may include altered level of awareness (not a typical stroke symptom but seen in bilateral thalamic ischaemia).[75]
Lacunar stroke syndromes
The following clinical features and physical examination findings are characteristic of the type of lacunar syndrome:
Pure motor hemiparesis |
|
Pure sensory stroke |
|
Ataxic hemiparesis |
|
Sensorimotor stroke |
|
Dysarthria-clumsy hand syndrome |
|
Take a careful history. Be sure to establish contact with witnesses or next of kin, not only for an accurate history but also to seek consent for invasive tests or treatments, if these are needed.
Determine the time of symptom onset because this is the main factor that will determine eligibility for thrombolysis.
If the onset was unwitnessed, the time of symptom onset is when the patient was last seen well.[67]
Ask about onset (sudden or gradual), duration, intensity, and fluctuation of symptoms.
The symptoms and signs of ischaemic stroke appear suddenly and are maximum at onset.
Patients with posterior circulation stroke may present with recurrent, stuttering, or progressive symptoms, which may include an altered level of consciousness.[75]
Ask specifically about relevant past medical history that will influence management. This includes (brief history):
Recent stroke
Seizure or epilepsy
Myocardial infarction
Atrial fibrillation
Recent surgery
Recent trauma
Bleeding
Haemorrhagic stroke
Comorbidities (specifically hypertension and diabetes)
Current or past illicit drug use
Medicines (specifically anticoagulants, insulin, and antihypertensives).
Practical tip
The time of onset is not always easy to determine, particularly if the onset was not witnessed and the patient is unable to communicate, if symptoms are mild and not immediately noticeable, or if there is a stuttering or fluctuating course.
Bear in mind key risk factors for ischaemic stroke:
Age ≥55 years
A strong non-modifiable risk factor, even after controlling for other age-related conditions such as hypertension.[11]
History of transient ischaemic attack (TIA)
Patients with a history of TIA, particularly a recent TIA, are at a significant risk of subsequent stroke. Most of these strokes occur within days of the TIA. Stroke rate has been reported as 1.5%, 2.1%, 2.8%, 3.7%, and 5.1% on days 2, 7, 30, 90, and 365, respectively, after TIA.[23] Studies show that the rate of post-TIA stroke might have decreased slightly since 1999, likely related to advances in cardiovascular risk prevention.[24][25]
History of ischaemic stroke
Indicates that the patient may have more ischaemic strokes in the future (particularly if risk factors such as hypertension are not corrected).[78]
Family history of stroke at young age
Stroke-causing genetic disorders with Mendelian inheritance are rare. Twin studies suggest a small genetic contribution to stroke; epidemiological studies show that family history of stroke is a risk factor.[21]
Hypertension
Strongly associated with an increased risk of ischaemic stroke.[79]
Smoking
Strongly associated with an increased risk of ischaemic stroke.[27]
Diabetes mellitus
Strongly associated with an increased risk of ischaemic stroke.[28]
Atrial fibrillation
Causes at least one fifth of ischaemic strokes and is one of the strongest individual stroke risk factors.[80]
Comorbid cardiac conditions
Including myocardial infarction, valvular disease, patent foramen ovale with or without atrial septal aneurysm, prosthetic heart valve, and cardiomyopathy.[30]
Sickle cell disease
Associated with vascular stenosis, brain ischaemia, and Moyamoya disease (vascular occlusion affecting the circle of Willis).
Dyslipidaemia
Increased total cholesterol is associated with an increased risk of ischaemic stroke. The risk of ischaemic stroke is decreased with elevated high-density lipoprotein (HDL) cholesterol.[81]
Exclude stroke mimics such as hypoglycaemia, brain tumours, seizures, sepsis, or migraine to ensure timely treatment. See Differentials.
Bear in mind the key clinical features that may help distinguish between stroke and mimics (e.g., seizures, hypoglycaemia) at the initial bedside assessment:
Suggestive of mimic | Suggestive of stroke |
|
Practical tip
Ischaemic stroke is a clinical diagnosis based on symptoms and signs. Therefore, distinguishing true stroke from mimics is an essential skill that cannot be replaced by imaging alone.
Assess the patient’s level of consciousness using the Glasgow Coma Scale. [ Glasgow Coma Scale Opens in new window ]
In people with an altered level of consciousness or coma, exclude haemorrhage and other mimics such as seizures. See Differentials.
Consider seizure (Todd’s paresis) in people with reduced consciousness.
Practical tip
Haemorrhagic stroke is more often associated with seizures, decreased level of consciousness, and signs of increased intracranial pressure than ischaemic stroke.
Perform an abbreviated neurological examination using the National Institutes of Health Stroke Scale.[69] [ NIH Stroke Score Opens in new window ]
This tool measures the degree of neurological deficits. Higher scores indicate a more severe stroke.
Check for evidence of cardiac arrhythmias (e.g., atrial fibrillation) or valvular pathology.
Auscultate the heart.
Arrhythmias, murmurs, and pulmonary oedema are associated with cardiac comorbidities, which predispose patients to stroke.
Transfer everyone with suspected stroke directly to a hyperacute (or acute, depending on availability) stroke unit as soon as possible; UK guidelines recommend doing this within 4 hours of presentation to hospital.[67]
CT head
Request brain imaging as soon as possible (at most within 1 hour of arrival at hospital).[68] Non-enhanced CT head is the investigation of choice in acute stroke.
Use the CT scan to differentiate between ischaemic stroke and haemorrhagic stroke; which must be done before starting thrombolysis in ischaemic stroke, and before reversing anticoagulation in anticoagulation-induced intracerebral haemorrhage.[68][83]
Only healthcare professionals with appropriate training should interpret acute stroke imaging for thrombolysis or thrombectomy decisions.[83]
Remember that ischaemic stroke is a clinical diagnosis based on signs and symptoms; a normal CT scan does not rule out a stroke - particularly in the first few hours, the CT scan can be normal or show very subtle ischaemic changes. A magnetic resonance imaging (MRI) scan in the presence of ongoing symptoms is extremely likely to show the stroke. A normal diffusion-weighted MRI scan is very unlikely if the patient has had a stroke.[84]
Practical tip
Ring through to a radiologist on call to advise an immediate scan; speak to the radiographer to ensure the patient has the next available time slot.
Aim to take a collateral history from relatives regarding medications/past medical history while the patient is in the scanner.
[Figure caption and citation for the preceding image starts]: Non-contrast CT scan of brain showing sub-acute isolated left basal ganglion infarction with left frontal horn mass effectCourtesy of BMJ Case Reports 2009; doi:10.1136/bcr.10.2008.1139 [Citation ends].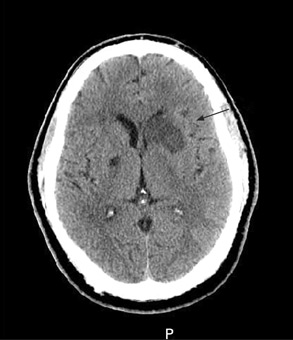
Diffusion-weighted MRI
Consider diffusion-weighted MRI of the head with stroke-specific sequences (DWI with SWI or T2*-weighted imaging) if the diagnosis remains uncertain despite CT head.[68]
Practical tip
An MRI scan in the presence of ongoing symptoms is extremely likely to show the stroke. A normal MRI scan is very unlikely if the patient has had a stroke.[84]
[Figure caption and citation for the preceding image starts]: (A) Non-contrast T1-weighted MRI. (B) Post-contrast T1-weighted MRI showing minimal increase in leptomeningeal vessels over the right frontal region. (C) Diffusion-weighted image (DWI) showing a hyperintense area in the right frontal region. (D) Apparent diffusion coefficient (ADC) map shows hypointense lesion, indicating restricted diffusion that correlates with high intensity on DWI and exponential diffusion. (E) ADC value is 0.22 x 10³ mm²/second, corresponding to a hyperacute infarctFrom the personal collection of Eric E. Smith; used with permission [Citation ends].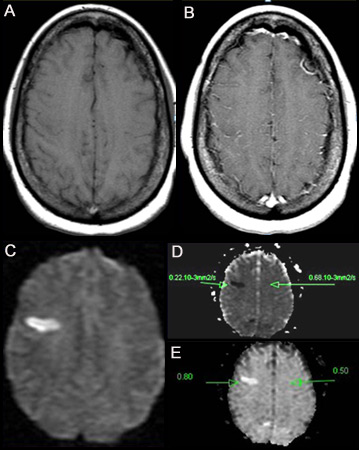
In candidates for endovascular thrombectomy
Patients presenting within 6 to 24 hours of symptom onset (i.e., from when they were last known to be well) may be potential candidates for endovascular thrombectomy.[67]
The selection of patients for mechanical thrombectomy (endovascular intervention) should be made by clinicians experienced in the use of thrombolysis for stroke and in interpretation of relevant imaging. The procedure should only be carried out by appropriately trained specialists with regular experience in intracranial endovascular interventions, with appropriate facilities and neuroscience support.[85]
CT angiography (CTA)
In patients with a suspected large vessel occlusion who are candidates for thrombectomy, request a CTA following the initial non-enhanced CT.[67][68]
Do not delay therapy with intravenous thrombolysis (if indicated) while waiting to perform CTA or waiting for results.[70] In practice, hospitals that undertake CTA routinely in acute stroke give thrombolysis without waiting for the CTA report; they review the initial plain CT at the same time as performing the CTA.[70]
Use CTA preferentially over MRA because CTA gives quicker results.[67]
In candidates for endovascular thrombectomy in addition to thrombolysis
CTA with contrast
If the patient is a potential candidate for thrombectomy in addition to thrombolysis, request CTA with contrast after (or with) the initial CT or MRI head to confirm occlusion of the proximal anterior or posterior circulation.[67][68]
CT perfusion imaging (or MR equivalent)
Add CT perfusion imaging (or MR equivalent) (at most within 1 hour of arrival at hospital) in patients with stroke with a delayed presentation for whom reperfusion is potentially indicated.[68] Studies have supported the use of perfusion scanning in patients to extend the thrombectomy window above 6 hours.[86][87][88] An alternative for patients who wake up with stroke is MRI measuring DWI-FLAIR mismatch.[68]
[Figure caption and citation for the preceding image starts]: MRI arterial spin labelling image showing extensive hypoperfusion in the right cerebral hemisphere. There is a clear mismatch between diffusion and perfusionFrom the personal collection of Eric E. Smith; used with permission [Citation ends].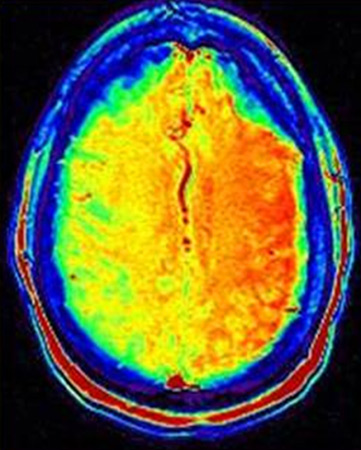
UK guidelines recommend thrombectomy (± thrombolysis) in patients who were last known to be well between 6 hours and 24 hours previously (including wake-up strokes) with confirmed occlusion of the proximal anterior or posterior circulation, if there is potential to salvage brain tissue as shown by perfusion imaging.[68]
In suspected carotid stenosis: carotid duplex ultrasound or CT angiography or MR angiography
Patients with ischaemic stroke who after specialist assessment are considered candidates for carotid intervention should have carotid imaging performed within 24 hours of assessment. This includes carotid duplex ultrasound or either CT angiography or MR angiography.[68] Consult your local protocol on choice of investigation. Carotid duplex ultrasound is most commonly used.
Practical tip
Request a chest x-ray in patients with cardiopulmonary signs or symptoms to detect other relevant conditions such as cardiomegaly, aortic dissection, or pneumonia.
Echocardiogram
If you suspect cardioaortic embolism, consider contrast transthoracic echocardiography (TTE) to evaluate the cardiac and aortic sources of embolus.[89] If no source is identified on TTE, use contrast transoesophageal echocardiography (TOE) in selected patients instead.[89]
Do not delay intravenous thrombolysis (if within the licensed time window and not contraindicated) while waiting for results or waiting to perform tests, unless you suspect contraindications that must be ruled out first (e.g., hypoglycaemia, coagulopathy).[70][71]
Blood tests
While CT/MRI transport is being organised, insert an intravenous catheter with blood sampling.[68]
Order in all patients:
Serum glucose
Serum electrolytes
To exclude electrolyte disturbance (e.g., hyponatraemia) as a cause for sudden onset of neurological signs.
Serum urea and creatinine
To exclude renal failure because it may be a potential contraindication to some stroke interventions.
Cardiac enzymes
To exclude concomitant myocardial infarction.
Full blood count
To exclude anaemia or thrombocytopenia prior to possible initiation of thrombolysis, anticoagulants, or antithrombotics.
Prothrombin time and partial thromboplastin time (with international normalised ratio)
To exclude coagulopathy.
Don’t delay thrombolysis (e.g., by waiting for test results) if the patient has no history of anticoagulant use, coagulopathy, or a condition that may lead to coagulopathy.[69]
Consider a serum toxicology screen if you suspect ingestion of toxic substances. Signs and symptoms may mimic stroke.
ECG
Perform an ECG in all patients to exclude cardiac arrhythmia (such as atrial fibrillation) or ischaemia, which are both relatively common in ischaemic stroke.[80]
Atrial fibrillation is an independent risk factor for ischaemic stroke and indicates a poor prognosis.[29] See New-onset atrial fibrillation.
In people who would be eligible for secondary prevention treatment for atrial fibrillation or flutter:[68]
Perform prolonged ECG monitoring (at least 24 hours)
Consider prolonged sequential or continuous ECG monitoring with an external patch, wearable recorder, or implantable loop recorder in those in whom no other cause of stroke has been found, particularly if they have a pattern of cerebral ischaemia on brain imaging suggestive of cardioembolism.
Practical tip
Atrial fibrillation is a major preventable cause of ischaemic stroke. Monitor all patients with suspected stroke for atrial fibrillation and other arrhythmias.[68] See New-onset atrial fibrillation.
The presence of paroxysmal atrial fibrillation has previously been underestimated, and latest guidance in the UK is to consider longer monitoring and implantable devices in more patients.[68][91]
Use of this content is subject to our disclaimer