Article Text

Statistics from Altmetric.com
In Western society, coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality. Extensive effort is continuously invested in the optimisation of diagnosing CAD and selecting subsequent treatment. Within this area, the role of non-invasive imaging has increased enormously. As compared with exercise ECG testing, visualisation of ischaemia using nuclear perfusion imaging (or stress echocardiography or magnetic resonance imaging) has considerably improved detection of CAD as well as appropriate selection of patients in need of further invasive evaluation. More recently, however, a new non-invasive imaging modality has been introduced, namely non-invasive computed tomography coronary angiography (CTA). In contrast to the traditional non-invasive imaging techniques, electron beam computed tomography (EBCT) and multi-slice computed tomography (MSCT) permit direct visualisation of the coronary arteries and stenoses. These techniques have attracted a lot of attention, since non-invasive assessment of coronary atherosclerosis and stenoses was previously not possible. The CT techniques have been validated against invasive coronary angiography, and excellent accuracy for detection of coronary artery stenoses was demonstrated in selected patient populations. For EBCT, pooled analysis of 538 patients demonstrated a mean sensitivity of 87% with a specificity of 91%.1 For 64-slice CT, a recent meta-analysis of six studies with 501 patients revealed even higher accuracies, with a mean sensitivity of 93% and specificity of 96% for the detection of significant stenoses.2 With the more recently introduced dual-source CT, accuracy may be even higher.3 Weustink and colleagues recently studied 100 symptomatic patients using dual-source CT and observed an excellent sensitivity and specificity of 95% for the detection of significant stenoses.
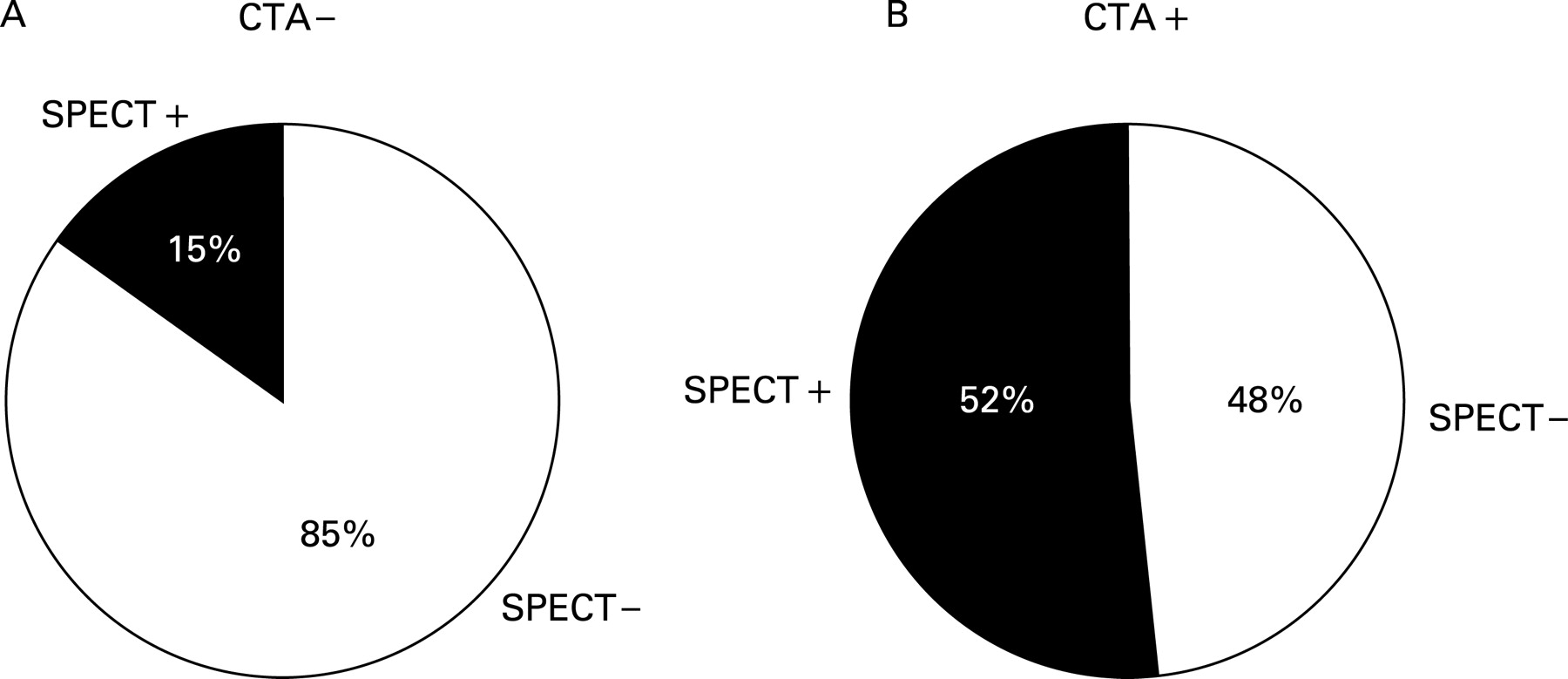
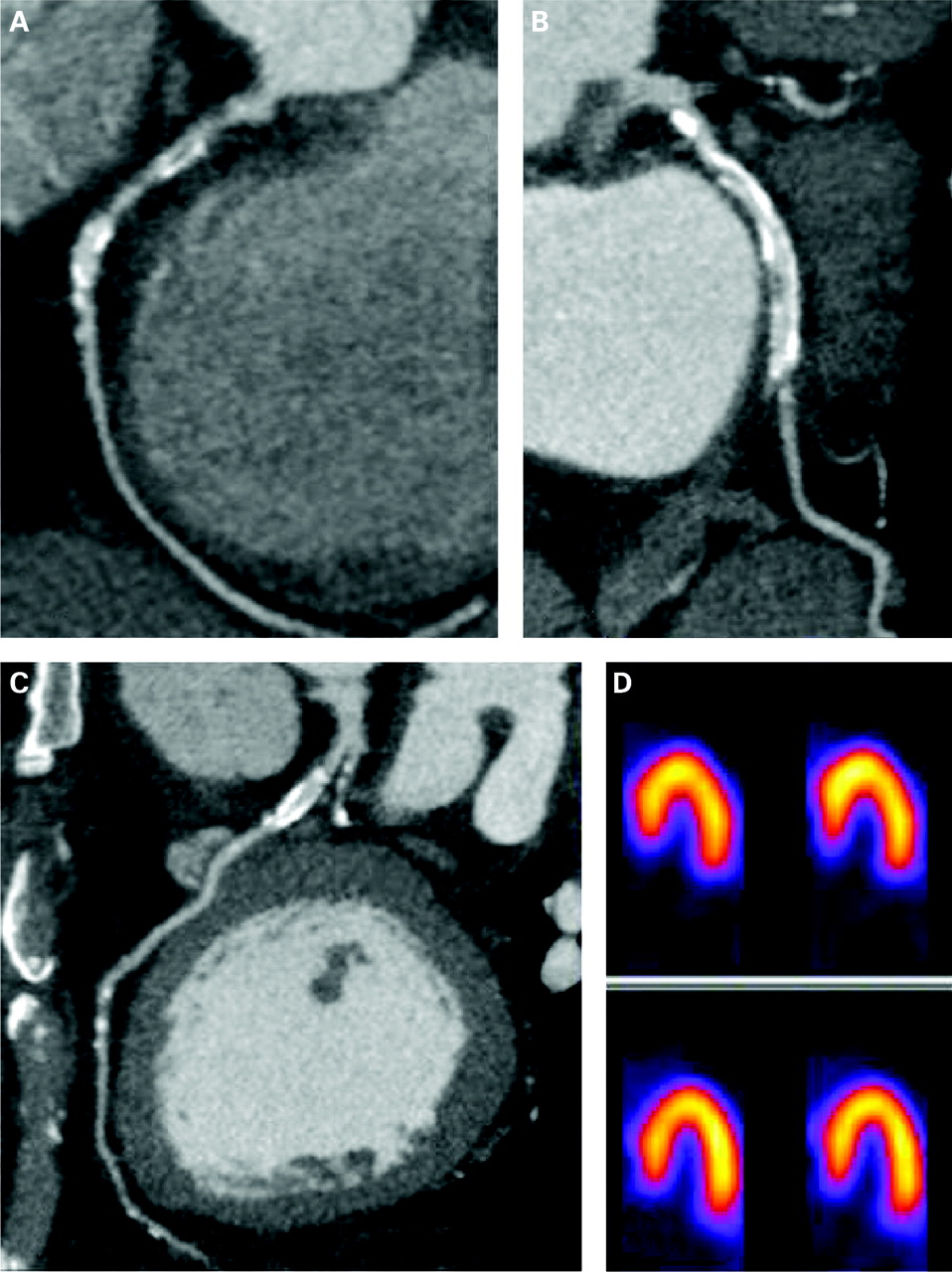
Despite this high accuracy, the precise position of CTA in clinical practice is not yet defined. Moreover, whether and when CTA may serve as an alternative to nuclear perfusion imaging (or any other imaging modality that detects ischaemia) is a topic of ongoing debate. In order to determine the relative merits of non-invasive coronary angiography and functional (ischaemia) testing, comparative studies are needed, and at present only a few head-to-head comparisons between CTA and nuclear perfusion imaging have been published (table 1). In general, a good agreement between modalities is reported in the case of a normal CTA.4–6 As illustrated in fig 1A, the vast majority of patients with a normal CTA (defined as the absence of ⩾50% stenosis) also show normal perfusion on single photon emission computed tomography (SPECT) imaging. These observations are in line with the high negative predictive value observed in comparisons of CTA with conventional coronary angiography,2 and indicate that a normal CTA is associated with a very low likelihood of clinically relevant CAD. Consequently, CTA may be used to rule out CAD and to identify those patients who may be discharged without further evaluation. However, a substantially lower agreement between the anatomical and functional approaches has been shown in patients with significant abnormalities on CTA4–6 (fig 1B). An example of a patient with an abnormal CTA with normal perfusion on SPECT is shown in figure 2.


Hacker et al,6 reporting observations in 38 patients (26 with suspected and 12 with known CAD), showed positive predictive values as low as 32% and 60% of 64-slice CTA to detect ischaemia on SPECT, on a vessel and patient basis respectively. Similar observations were reported in a larger study dedicated to patients with an intermediate pretest likelihood of CAD.4 In patients with at least one lesion with ⩾50% luminal narrowing, abnormal perfusion was noted in only 20 (50%) of 40 patients. Accordingly, in line with earlier comparisons between invasive coronary angiography and functional testing,7 8 these data suggest that only a modest relation between CTA and myocardial perfusion imaging exists. These data underscore that only a subset of significant lesions on CTA result in ischaemia (fig 1B).4–6 Indeed, the percentage stenosis may at best be only a moderate predictor of perfusion abnormalities. Other factors that may influence myocardial perfusion, such as plaque morphology and endothelial function, are not accounted for by stenosis severity.
Since the decision for revascularisation is frequently based on detection of stress-inducible ischaemia, functional imaging remains essential for appropriate selection of therapy (medical versus invasive evaluation with possible revascularisation) in patients with significant CAD on CTA.
On the other hand, in subjects with a normal perfusion study, CTA allows further differentiation into patients with atherosclerosis and patients with completely normal coronary arteries.4 9 This differentiation may permit identification of CAD at an earlier stage, namely while atherosclerotic changes are present, although still without haemodynamic consequences. These patients lack ischaemia, and thus have good prognosis and do not require immediate revascularisation; still, they benefit from aggressive medical therapy (statins, aspirin) and risk factor modification as well as close monitoring and follow-up. Particularly in certain subpopulations in which conventional stress-testing would underestimate risk, such as patients with diabetes or metabolic syndrome, detection of subclinical atherosclerosis may offer a substantial advantage. Thus, the combination of perfusion imaging and CTA appears to provide a promising opportunity to enhance diagnosis and selection of therapy in patients with suspected CAD.10 11
Further refinement in the integrated use of perfusion imaging and CTA may be guided by the pretest likelihood of CAD. In patients with a high pretest likelihood of CAD, the incremental value of CTA may be limited. Since the prevalence of CAD in this population is high, direct referral to invasive coronary angiography is usually preferred. In patients with a very low pretest likelihood of CAD, no imaging should be performed. The main benefit is in patients with an intermediate pretest likelihood of CAD; in these patients CTA could be used as a first step to determine the absence or presence of atherosclerosis. In the case of minimal, non-obstructive atherosclerosis on CTA, no functional testing is indicated and medical therapy/risk factor modification is indicated. In case of severe abnormalities on CTA (eg, 3-vessel or left main disease) functional imaging is also not needed, but referral to invasive coronary angiography and possible intervention should be considered.
Further evaluation by functional imaging following CTA is, however, needed in patients with intermediate, diffuse lesions on CTA; in these patients the presence or absence of ischaemia will determine whether invasive evaluation is indicated. This potential algorithm is summarised in figure 3.

{kind=link}
{kind=link}
{kind=link}
In conclusion, integrated use of anatomical imaging (to assess atherosclerosis) will permit further refinement in evaluation of patients with suspected CAD. The precise roles of both techniques need further evaluation in large, prospective studies that address long-term follow-up and cost-effectiveness.
REFERENCES
Footnotes
Competing interests: Jeroen J Bax has research grants from GE Healthcare and BMS Medical Imaging.