Article Text

Abstract
Objectives We sought to clarify the variations in the anatomy of the superior cavoatrial junction and anomalously connected pulmonary veins in patients with superior sinus venosus defects using computed tomographic (CT) angiography.
Methods CT angiograms of 96 consecutive patients known to have superior sinus venosus defects were analysed.
Results The median age of the patients was 34.5 years. In seven (7%) patients, the defect showed significant caudal extension, having a supero-inferior dimension greater than 25 mm. All patients had anomalous connection of the right superior pulmonary vein. The right middle and right inferior pulmonary vein were also connected anomalously in 88 (92%) and 17 (18%) patients, respectively. Anomalous connection of the right inferior pulmonary vein was more common in those with significant caudal extension of the defect (57% vs 15%, p=0.005). Among anomalously connected pulmonary veins, the right superior, middle, and inferior pulmonary veins were committed to the left atrium in 6, 17, and 11 patients, respectively. The superior caval vein over-rode the interatrial septum in 67 (70%) patients, with greater than 50% over-ride in 3 patients.
Conclusion Anomalous connection of the right-sided pulmonary veins is universal, but is not limited to the right upper lobe. Not all individuals have over-riding of superior caval vein. In a minority of patients, the defect has significant caudal extension, and anomalously connected pulmonary veins are committed to the left atrium. These findings have significant clinical and therapeutic implications.
- computed tomography angiography
- heart defects
- congenital
- heart septal defects
- atrial
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Introduction
The superior sinus venosus defect is the most common interatrial communication outside the oval fossa. It is characterised by anomalous connection of one or more of the right-sided pulmonary veins. The orifice of the superior caval vein usually over-rides the atrial septum, but is not universal (figure 1).1–4 Surgical repair is the standard of care.5 More recently, transcatheter closure has been introduced as an option for correction, placing a covered stent in the superior caval vein with its lower end in the right atrium flared to close the defect, simultaneously redirecting the right-sided pulmonary veins into the left atrium.6–8 Detailed knowledge of the anatomy of cavoatrial junction and arrangement of right-sided pulmonary veins is crucial for optimal closure, the more so if transcatheter closure is contemplated. The anatomy of the superior cavoatrial junction, and the location of right-sided pulmonary veins, however, are far from constant.2 9–11 To the best of our knowledge, as yet no studies have been performed to provide a detailed account of all these anatomical features.1 2 4 12 We, therefore, sought to clarify these anatomical features using CT angiography.

Illustration compares the anatomy of a normal heart (A) with a heart with superior sinus venosus defect (B). Interatrial communication in the superior sinus venosus defect is outside the oval fossa. The superior caval vein (SCV) has a variable degree of over-ride relative to the interatrial septum, and the right-sided pulmonary veins are connected anomalously in the region of the superior cavoatrial junction.
Methods
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Following approval from institutional ethics committee, we included all consecutive patients with superior sinus venosus defect older than 14 years, who had undergone preoperative scanning between January 2016 and August 2020. We excluded patients with concomitant significant congenital heart diseases, other than a coexisting defect within the oval fossa. The CT datasets were independently analysed by a paediatric cardiologist and two cardiac radiologists. The differences were resolved by consensus, with inputs from another paediatric cardiologist. The demographic details were obtained from medical records.
Acquisition and analysis of the CT datasets
The CT angiograms had been acquired with retrospective electrocardiographic gating on either a 256-slice or 384-slice dual-source scanner (Siemens Healthcare, Germany), using an intravenous injection of 1.5 mL/kg iodinated contrast followed by a half-saline chase. The recirculation phase was assessed to delineate venous anatomy. A Syngovia workstation (Siemens Healthcare, Germany) was used for multiplanar reformatting, with maximal and minimal intensity projection formats. These interrogations were supplemented by virtual dissection of volume-rendered datasets using open-source Horos software (Pixmeo, Switzerland) on a Macintosh computer.13
Anatomical assessment
After evaluating the segmental cardiac anatomy, we confirmed defects to be outside the confines of the oval fossa, and adjacent to the superior caval vein. By aligning a reference line along the interatrial septum to obtain an oblique sagittal or left anterior oblique view, we measured the maximum supero-inferior dimension of the defect from its superior margin to the superior rim of the oval fossa (figure 2A and C). An orthogonal modified axial view, equivalent to a right anterior oblique projection, then provided the maximum transverse dimensions of the defect from its anterior margin to the posterior atrial wall (figure 2B,C). Defects with a supero-inferior dimension greater than 25 mm were deemed to have significant caudal extension, basing this on the length of the right atrial portion of the covered stent used most frequently in 25 patients undergoing transcatheter closure, reported by Hansen et al.6

CT angiographic images from a patient with a superior sinus venosus defect. (A) The oblique sagittal view was used to measure the supero-inferior (blue arrow) dimension of the defect. (B) The modified axial view was used to measure transverse (green arrow) dimension of the defect. (C) Virtual dissection of the defect in the right anterior oblique view with cranial angulation provides an ’en face’ view of the defect and its relationship with the anomalously connected right superior pulmonary vein (yellow star). There is an additional oval fossa defect (ASD). Ao, aorta; ASD, atrial septal defect; CS, coronary sinus; ICV, inferior caval vein; LA, left atrium; PT, pulmonary trunk; RA, right atrium; RPA, right pulmonary artery; RV, right ventricle; SCV, superior caval vein.
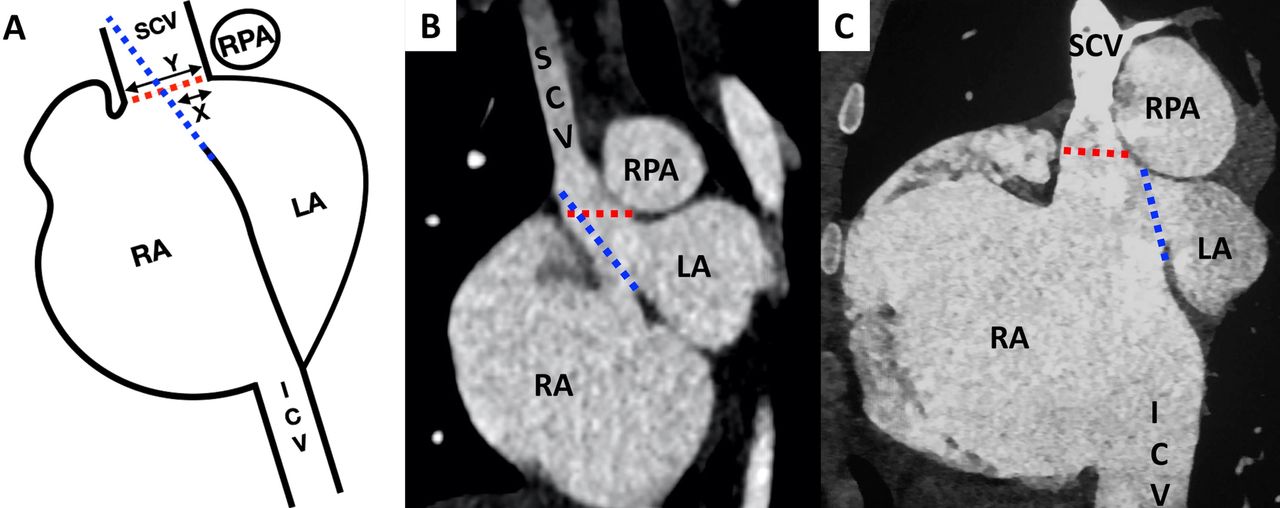
The diameter of the superior caval vein was assessed in the oblique sagittal plane, revealing the degree of its over-ride relative to the superior rim of the oval fossa (figure 3A). We also measured its diameter between the level of the most superiorly connected right superior pulmonary vein, and the level of drainage of the azygos vein. The over-ride was assessed in a fashion analogous to that used for the aortic root in tetralogy of Fallot,14 classifying it as none, less than 50%, or more than 50% when the greater part of the caval vein was committed to the left atrium. If present, we also measured the diameter of the left-sided superior caval vein. We identified the individual pulmonary veins from all the bronchopulmonary segments of both lungs, noting the site of their atrial connections relative to the plane of the atrial septum. Segmental connection was considered different if veins from different bronchopulmonary segments of the same lobe connected to multiple sites.15

The method of assessing degree of over-ride of right superior caval vein (SCV), with examples. (A) The line diagram shows the defect in the oblique sagittal plane. The interatrial septum is first projected cranially (blue broken line), and the measurements are performed at the superior cavoatrial junction (red broken line). The degree of over-ride is measured as the ratio of SCV (at cavoatrial junction) lying behind the projected interatrial septum (X) to the diameter of SCV at the cavoatrial junction (Y). (B) The patient has greater than 50% over-ride of the SCV. (C) The patient has no over-ride of the SCV. ICV, inferior caval vein; LA, left atrium; RA, right atrium; RPA, right pulmonary artery.
The anomalous connection of the right pulmonary veins in the environs of the defect meant that it was no longer possible to identify a clear demarcation between the atrial chambers.7 16 17 For management, however, the precise atrial commitment of the pulmonary veins is important. We assessed, therefore, the precise proportions of their orifices committed to the left or the right atrium relative to the plane of the atrial septum in the modified axial view. This permitted us to distinguish between those veins with the entirety of their orifice committed to the left, as opposed to those with the orifice committed to the right of atrial septum (online supplemental figure).
Supplemental material
We considered pulmonary veins to be connected to the superior cavoatrial junction if their orifices were within 5 mm of the junction of superior caval vein with the right atrium. In view of potential implications for surgical and interventional closure,6–8 18 pulmonary veins were considered to have high connection if the upper border of their orifice was greater than 2 cm cranial to the superior cavoatrial junction. This definition included additional pulmonary veins connected directly to the superior caval vein more than 2 cm above the superior cavoatrial junction. We measured the diameter of pulmonary trunk and identified any compression of the left coronary artery. We also assessed the pulmonary parenchyma and airways.
Statistical analysis
Categorical data were represented by percentages or frequencies and were compared using Fisher’s exact tests. Continuous variables were summarised as median with range, or mean with SD and were compared using independent samples t-test. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS V.23 software (IBM).
Results
We analysed CT datasets from 96 individuals with a median age of 34.5 years (table 1). All had normal sequential segmental anatomy. The defects measured 19.4±5.4 mm transversely, and 18.0±4.9 mm in their supero-inferior extent. In 67 (70%) patients, the superior caval vein was over-riding the atrial septum, but in only 3 was it committed predominantly to the left atrium. A left superior caval vein, draining through the coronary sinus, was present in 18 (19%) patients. The right superior caval vein was narrower in these patients, measuring 10.6±1.7 mm as opposed to 15.1±2.5 mm (p<0.001). The transverse and supero-inferior dimensions of the defects, however, were not different (online supplemental table).
Supplemental material
Demographic and anatomical characteristics (n=96)
We found marked variation in the patterns of pulmonary venous drainage. In 48 individuals, the right upper lobe drained through one vein, through two veins in 46, and through three veins in 2 patients. The right middle lobe drained through a single vein in 76 individuals (79%), and through two veins in 20 (21%). The right lower lobe drained through a solitary vein in 85 (89%) patients, through two veins in 10 (10%) and through three veins in 1 individual. Taken overall, there were a total of 146 right superior, 116 right middle and 108 right inferior pulmonary veins.
In terms of the pulmonary venous connections, apart from one patient with the left superior pulmonary vein connecting to the left superior caval vein, all left pulmonary veins were normally connected. With regard to the right-sided veins, the right superior pulmonary vein was anomalously connected in all. In 88 (92%) patients, there was anomalous connection of the right middle pulmonary vein, with 17 (18%) patients also having anomalous connection of the right inferior pulmonary vein. Such anomalous connection of the right inferior pulmonary vein was more frequent in those with significant caudal extension of the defect (57% vs 15%, p=0.005). In 20 (21%) patients, the right middle pulmonary veins formed a confluence with the other veins, joining with the superior vein in 15, and the inferior vein in 5. In two of the five patients having a confluence with the right inferior pulmonary vein, the venous orifice was committed exclusively to the left atrium.
Among veins connected anomalously, the right superior pulmonary veins were committed to the left atrium in 6 (6%) patients, while in 90 (94%) they were committed to the right atrium, including patients with direct connection away from the superior cavoatrial junction. In contrast, the right middle and inferior pulmonary veins were committed to the left atrium in 17 and 11 individuals, respectively. The defect was smaller in patients with left atrial commitment of the right superior pulmonary vein compared with those with right atrial commitment. The size of the defect, however, was not different in those with anomalously connecting middle and inferior veins, irrespective of their relationship to the plane of the atrial septum (online supplemental table).
The anomalous pulmonary veins were connected high in the superior caval vein in 57 (59%) patients, including 34 patients in whom a small vein drained only a single bronchopulmonary segment, and 14 patients in whom the veins drained more than one lung segment. In the remaining nine patients, the orifice of anomalous vein was large, and extended more than 2 cm cranially from the cavoatrial junction.
Differences in segmental connections of the pulmonary veins were identified in 36 (38%) patients. In 31 of these, despite the differences in the connections, veins draining all segments of the lobe emptied into the right atrium (figure 4A). In the remaining five, some of the segments were connected to the left atrium, while others connected to the right atrium (figure 4B,C).

CT angiographic images showing the differences in segmental pulmonary venous connections. (A) The coronal section shows the vein from the apical segment (red arrow) of the right upper lobe connecting directly to the superior caval vein (SCV), while veins from the rest of the segments (red star) connect to the right atrium at the superior cavoatrial junction. (B) Axial section from another patient shows veins from the apical and posterior basal segments of the right lower lobe (red arrow) over-riding the interatrial septum across the sinus venosus defect. (C) Axial section from the same patient as (B) showing rest of the segments of the right lower lobe connecting to the left atrium. Ao, aorta; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
A defect within the oval fossa coexisted in 16 patients. Pulmonary parenchymal abnormalities, such as bilateral mosaic attenuation, bronchiectasis, emphysematous changes, fibro-atelectatic bands and consolidation, were found in 43 (45%) patients. The sinus venosus defects were larger in the individuals with abnormal pulmonary parenchyma, having a transverse dimension of 20.9±6.2 mm as opposed to 18.2±4.5 mm in those without such abnormalities (p=0.02). The comparable supero-inferior diameters were 19.1±4.9 mm vs 17.1±4.8 mm (p=0.05) (online supplemental table). None of the patients had compression of the airways. Compression of the left coronary artery by the pulmonary trunk was present in six (6%) individuals. These patients had larger pulmonary trunk, measuring 43.4±7.9 mm as opposed to 34.3±7.8 mm (p=0.007). The size of sinus venosus defects, however, was not different in these two groups.
Discussion
Although initially described more than 150 years ago, the anatomy of the superior sinus venosus defect remains poorly understood.1 2 4 10 12 19–21 There is general agreement that anomalous connection of the right-sided pulmonary veins is an essential phenotypical feature. Although increasingly accepted that the defect has an extraseptal location, it remains common to find the lesion being incorrectly described as an ‘atrial septal defect’.6 The precise anatomy, furthermore, remains a matter of debate. In part, this reflects the difficulty in assessing all the anatomical features with precision by echocardiography, during surgery or even while examining autopsied specimens.2 9 21 The problems also reflect lack of standard definitions, and the use of different modalities for evaluation (table 2).4 12 21–24 We chose to use CT angiography because of its high spatial resolution, and its ability to provide excellent three-dimensional visualisation of the superior cavoatrial junction.13
Comparison of index study with the published studies
Anomalous connection of the right-sided pulmonary veins to the atrial chambers is now accepted as the phenotypical feature of the defect, although with no clarity on this aspect among even those using this definition.2 10 The exact frequency and extent of anomalous connection of the right-sided pulmonary veins is also not well described (table 2).4 9 21–24 Further, the terms ‘anomalous connection’ and ‘anomalous drainage’ have been used interchangeably, although without the use of flow-based studies to clarify drainage. Despite a predominant left atrial connection, a pulmonary vein can still drain anomalously if its orifice lies close to the defect.16 17 In the absence of flow studies to define drainage, we chose to define left or right atrial commitment of anomalously connected pulmonary veins relative to the plane of the atrial septum. When assessed using this criterion, a majority of patients had the right superior pulmonary vein committed to the right atrium. A significant proportion also had the right middle and inferior pulmonary veins committed to the right atrium. It is intuitive that a pulmonary vein with left atrial commitment is less likely to become obstructed during transcatheter closure (online supplemental figure).6–8 On the other hand, pulmonary veins committed to the right atrium, either in relation to the cavoatrial junction or away from it, are more likely to suffer obstruction during placement of a covered stent. Even in these situations, nonetheless, a spacious cavoatrial junction may still permit placement of a covered stent without inducing pulmonary venous obstruction (figure 5A,B). The situation differs during surgical repair, where the surgeon uses a flexible patch to redirect the pulmonary veins to the left atrium, while at the same time reconnecting the caval vein to the right atrium. Surgeons, therefore, have greater ability to manage our observed variations. Connection of the pulmonary veins at a distance from the superior cavoatrial junction, nevertheless, will mandate modification in the surgical repair technique in some cases.5

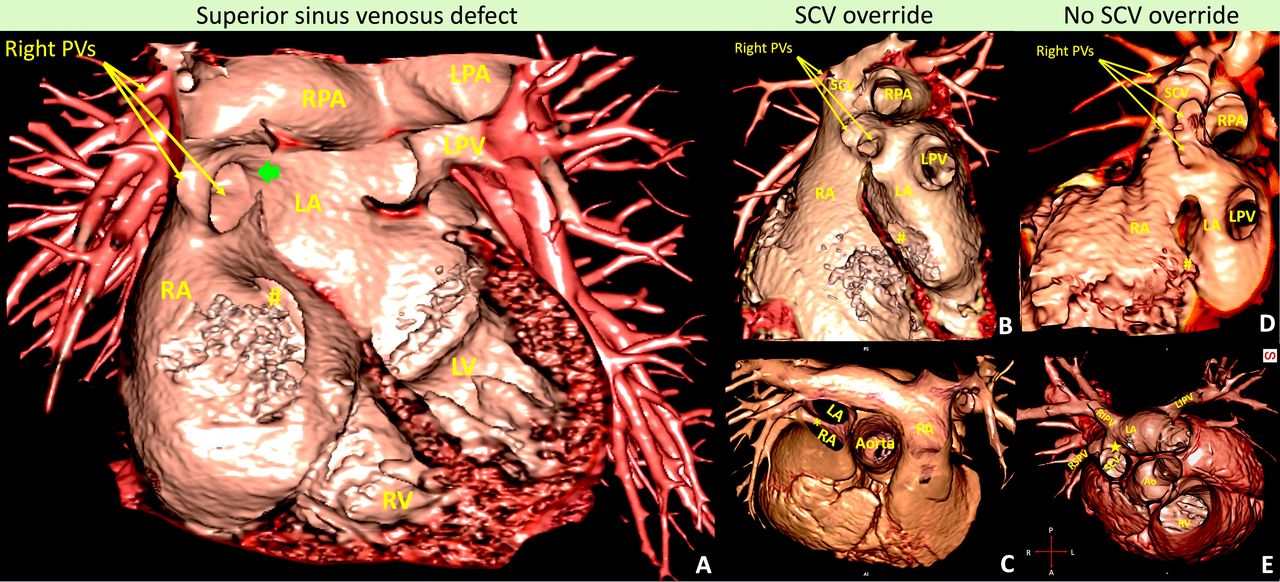
Virtual dissection images from CT angiograms showing the anatomy of the superior sinus venosus defect. (A) The classic defect in the region of superior cavoatrial junction (green block arrow), with the defect located outside the oval fossa. Right-sided pulmonary veins are connected anomalously in the region of the defect. An additional pulmonary vein is seen connected directly to the SCV. (B and C) The anatomy, in long axis and short axis view, respectively, of the superior cavoatrial junction from a patient with SCV over-riding the interatrial septum (*). (D and E) Corresponding views from a patient without over-ride (★). An atrial septal defect (#) is also seen. Ao, aorta; LA, left atrium; LIPV, left inferior pulmonary vein; LPA, left pulmonary artery; LPV, left pulmonary vein; LV, left ventricle; PV, pulmonary vein; RA, right atrium; RIPV, right inferior pulmonary vein; RPA, right pulmonary artery; RSPV, right superior pulmonary vein; RV, right ventricle; SCV, superior caval vein.
Unlike the normal population, where two-thirds of individuals have their right middle lobe draining to the left atrium through either the superior or inferior pulmonary veins,25 in only one-fifth of our cohort was the right middle lobe draining via the superior or inferior pulmonary veins. A difference in segmental connection of the veins, an observation of uncertain significance,15 was seen in one-third of our patients. These features likely reflect the abnormal development of both the pulmonary veins and the cavoatrial junction in the setting of the sinus venosus defect.
Unlike defects within the oval fossa, the sinus venosus defect is not merely a hole (figure 6). The deficiency at the superior cavoatrial junction, along with the abnormally connected pulmonary veins, creates a cone of space between the mouth of the superior caval vein and the superior rim of the oval fossa.4 9 19 The resulting variable over-ride of the caval vein is comparable with the aortic over-ride seen in the setting of tetralogy of Fallot (figure 6). The left posterior aspect of the cone of space is closed to re-establish unobstructed drainage of the superior caval vein to the right atrium, and the pulmonary veins to the left atrium. Currently, there is no standard method for measuring the extent of caval venous over-ride.1 4 19 26 Using the same approach as used for aortic over-ride in tetralogy of Fallot, we found no over-ride in one-third of our patients (figures 3C and 5C). Even among those with over-riding (figures 3B and 5A), in only three was the over-ride greater than 50%. This is consistent with the observations by Hsu et al, who found only minor over-riding in few of their 40 patients.21 A certain degree of caval venous over-ride is likely to be helpful for transcatheter closure, since it could facilitate apposition of covered stent to the atrial septum. Lack of over-ride, on the other hand, may explain the residual flow observed in some cases following implantation of covered stents.6 8 27

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Virtual dissection images comparing the anatomy of the superior sinus venosus defect with tetralogy of Fallot. (A) The anatomy in the sinus venosus defect is similar to the arrangement of the ventriculo-aortic junction in tetralogy of Fallot. As in tetralogy, it is the left posterior aspect of the cone of space that is closed, and not the so-called sinus venosus defect. Unlike tetralogy, however, it is the left atrial side of the cone of space that is closed when the surgeon diverts the right-sided pulmonary veins to the left atrium. (B) The ventriculo-aortic junction in tetralogy of Fallot. LA, left atrium; LPV, left pulmonary vein; LV, left ventricle; PV, pulmonary vein; RA, right atrium; RPA, right pulmonary artery; RV, right ventricle; SCV, superior caval vein.
In nearly one-fifth of our patients, we found a coexisting left superior caval vein. A similarly high prevalence has been reported previously1 23 28 being higher than 10% prevalence with other cardiac malformations.29 The right-sided superior caval vein was narrower in those patients with persistent left superior caval vein, although the size of the defect was not different in the two groups. A smaller right superior caval vein may be advantageous for those opting for interventional closure, permitting the use of covered stents of smaller diameter. It may also be a limitation in patients with larger defects, when greater flaring of the right atrial portion of the stent is needed to achieve complete closure of the atrial portion of the defect. The higher prevalence of oval fossa defects in our patients possibly indicates selection bias related to retrospective selection of cases.30
In recent years, interest in transcatheter closure has waxed.6–8 10 27 The anatomical criteria for suitability of such closure, however, are still evolving.6 8 Large size, significant caudal extension, and the potential for pulmonary venous obstruction currently preclude the transcatheter option.6–8 An additional vein connecting high in the superior caval vein is not currently considered a contraindication unless it is large, drains more than one lung segment and can be rerouted surgically. Pulmonary venous obstruction during transcatheter closure, nonetheless, is variable. Hansen et al,6 for example, reported pulmonary venous obstruction in less than 10% of their 28 patients. Sivakumar et al,8 in contrast, witnessed it in one-third of their 44 patients.8 Based on advanced imaging techniques, and the potential risk of obstruction, Tandon et al deemed one-fifth of 28 potential candidates unsuitable for transcatheter closure, while considering another quarter equivocal.7 Based on these principles, we would judge 26 (27%) of our patients suitable and 32 (33%) patients unsuitable for transcatheter closure. The remaining 38 (40%) individuals would be considered equivocal. We believe that the current difficulties encountered in assessing the risk of pulmonary venous obstruction reflect the challenges remaining in precise assessment of the anatomy of cavoatrial junction and the right-sided pulmonary veins. Analysis based on CT angiography, as we have shown, could well enhance decision-making for those contemplating transcatheter closure.
Limitations
We included only those patients who had undergone CT angiography. We also lack any clinical, haemodynamic or surgical correlation of our morphological findings. We accept, furthermore, that our assessment of commitment of the right-sided pulmonary veins and the superior caval vein as well as feasibility of transcatheter closure was based exclusively on anatomical principles.
Conclusion
Anomalous connection of the right-sided pulmonary veins is seen in all, but is not limited to the right upper lobe. Over-riding of the superior caval vein is not universal, being present in only two-thirds of patients. In a minority of patients, the defect has significant caudal extension and anomalously connected pulmonary veins are committed to the left atrium. These anatomical findings have important implications for those planning closure of the defects, more so if interventional closure is contemplated.
Key messages
What is already known on this subject?
The superior sinus venosus defect is the most common interatrial communication found outside the confines of the oval fossa. As yet, however, the precise connections of all the right-sided pulmonary veins remain to be clarified.
What might this study add?
Anomalous connection of the right-sided pulmonary veins is seen in all patients. The anomalous connection is not limited to right superior pulmonary veins, but is frequently seen with the right middle and inferior pulmonary veins as well. The over-riding of the superior caval vein is not universal.
How might this impact on clinical practice?
Our findings clarify the anatomical features of superior sinus venosus defect, showing how analysis of CT angiogram can provide optimal preprocedural planning for either transcatheter or surgical closure of the defect.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drsaurabhmd101, @rengadr
Contributors All of the authors contributed to one or more of the following: conception of design of the work (JR, SKG), data collection (JR, SKG, RR), data analysis and interpretation (JR, SKG, RR, GSG), drafting the manuscript (JR, SKG) and critical revision of the manuscript (all authors). All authors provided final approval of the manuscript. SKG and JR are responsible for the overall content as guarantors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in the submitted article by the authors are their own and not an official position of the institution.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.