Article Text

Abstract
Objective Commercial airplanes fly with an equivalent cabin fraction of inspired oxygen of 0.15, leading to reduced oxygen saturation (SpO2) in passengers. How this affects children with complex congenital heart disease (CHD) is unknown. We conducted Hypoxic Challenge Testing (HCT) to assess need for inflight supplemental oxygen.
Methods Children aged <16 years had a standard HCT. They were grouped as (A) normal versus abnormal baseline SpO2 (≥95% vs <95%) and (B) absence versus presence of an actual/potential right-to-left (R–L) shunt. We measured SpO2, heart rate, QT interval corrected for heart rate and partial pressure of carbon dioxide measured transcutaneously (PtcCO2). A test failed when children with (1) normal baseline SpO2 desaturated to 85%, (2) baseline SpO285%–94% desaturated by 15% of baseline; and (3) baseline SpO275%–84% desaturated to 70%.
Results There were 68 children, mean age 3.3 years (range 10 weeks–14.5 years). Children with normal (n=36) baseline SpO2 desaturated from median 99% to 91%, P<0.0001, and 3/36 (8%) failed the test. Those with abnormal baseline SpO2 (n=32) desaturated from median 84% to 76%, P<0.0001, and 5/32 (16%) failed (no significant difference between groups). Children with no R–L shunt (n=25) desaturated from median 99% to 93%, P<0.0001, but 0/25 failed. Those with an actual/potential R–L shunt (n=43) desaturated from median 87% to 78%, P<0.0001, and 8/43 (19%) failed (difference between groups P<0.02). PtcCO2, heart rate and QT interval corrected for heart rate were unaffected by the hypoxic state.
Conclusions This is the first evidence to help guide which children with CHD need a preflight HCT. We suggest all children with an actual or potential R–L shunt should be tested.
- airflight
- airplane
- hypoxia
- congenital heart disease
Statistics from Altmetric.com
Introduction
The PaO2 of inspired oxygen falls as altitude increases; commercial aircraft fly at 30 000–40 000 feet (9144–12 192 m), which would give an equivalent fraction of inspired oxygen (FiO2) of just 0.04. To combat this, aircraft cabins are pressurised, but only to a pressure equivalent altitude of 8000 feet (2438 m), which in turn leads to an FiO2 equivalent of 0.15 (rather than sea level 0.21).1 The oxygen saturation levels of healthy adults and children fall during airflight, by a mean of about 4%,2 3 although one study of crew members found the mean lowest arterial oxygen saturation measured by pulse oximetry (SpO2) fell from 97% before takeoff to 89% when flying (ranging from 80% to 93%).4 Hypobaric hypoxia can be a potential problem for some people with cardiorespiratory disease unless supplemental oxygen is provided, and there are established methods for preflight testing: the Hypoxic Challenge Testing, previously known as the Fitness to Fly test.5 6
Parents of children with congenital heart disease frequently wish to know if their child can fly safely for a holiday, and additionally some children fly abroad on commercial flights for surgical treatment. A recent systematic review concluded that current evidence meant it was not possible to give an appropriate evidence-based risk analysis for patients with congenital heart disease and airflight.7 There are 2011 guidelines from the British Thoracic Society on how to manage passengers with respiratory disease that includes those with cardiac comorbidity, but they simply state physicians should use their discretion in deciding whether to perform Hypoxic Challenge Testing and/or advise inflight oxygen for patients with cyanotic congenital heart disease.6 The British Cardiovascular Society 2010 guidelines are principally concerned with adult cardiac disease but include a section on cyanotic congenital heart disease,8 although the evidence on which their recommendations are based is from two small adult studies.9 10 The US Aerospace Medical Association Medical Guidelines for Airline Travel published in 2003 simply listed cyanotic congenital heart disease as an indication for medical oxygen during commercial airline flights, without any further clarification.11 Their more recent online guidance simply refers to the British Cardiovascular Society 2010 guidelines.12 The Canadian Paediatric Society 2007 guidelines, reaffirmed in 2016, make one brief statement that Eisenmenger syndrome in children is a contraindication to commercial airline flight.13
The aim of this study was to conduct Hypoxic Challenge Testing in children with complex heart disease, including those with univentricular physiology, in order to ascertain whether the test was feasible in these children. Assessing who desaturated and by how much would then provide guidance as to which children need a preflight assessment.
Methods
Subjects
Children with congenital heart disease were recruited from outpatient clinics and the ward at the Royal Brompton Hospital. Inclusion criteria were children aged <16.0 years with complex acyanotic or cyanotic congenital heart disease. Exclusion criteria were baseline SpO2 <75%, duct-dependent lesions, known pulmonary hypertension, pre-existing oxygen requirement or concomitant significant respiratory disease that would affect oxygenation. Children were subdivided into those with normal baseline SpO2 of 95% or above, or low baseline SpO2 75%–94%. Children were further categorised into whether their cardiac condition was unrepaired, repaired or treated with palliative surgery and also whether there was any actual or potential intracardiac right to left shunt at the time of the test.
Written informed consent was taken at the time of the test from the parents/carers and assent from the older children.
Hypoxic Challenge Testing
A paediatric cardiac doctor was present throughout the procedure. The child (and when necessary also the parent/carer) sat inside a sealed body plethysmograph.5 The following were monitored:
Functional SpO2 using two Masimo Radical 7 pulse oximeters (Masimo UK, Basingstoke, UK) attached to the child’s hand or foot. SpO2 was continuously recorded when there was a stable reproducible trace (excluding artefact), and the child was not moving too much.
Heart rate was recorded continuously via the ECG leads (see below), and the test level was taken at the time of the lowest SpO2 at FiO2 0.15.
Partial pressure of carbon dioxide was measured transcutaneously (PtcCO2) by continuous recordings using a TINA TCM44 monitor (Radiometer, Crawley, UK). This was to check if the child was hyperventilating to compensate for the hypoxic conditions, and a PtcCO2 <3.5 kPa was considered low and indicative of hyperventilation.
Standard ECG leads were connected (using MAC5500 ECG System, GE Healthcare, Hatfield, UK) and a recording printed at baseline and at FiO2 0.15 to measure the QT interval. This was taken from the hand-read mean of four readings from Lead II and V5 using Bazett’s formula to correct for heart rate (QT interval corrected for heart rate (QTc)). The cut-off for prolonged QTc was taken as ≥480 ms in the absence of a secondary cause for prolongation.14
Total haemoglobin measured by pulse co-oximetry (SpHb) was measured non-invasively using Masimo Radical 7 pulse co-oximetry.
Once settled, baseline readings were made in room air, and then the oxygen level inside the box was reduced over 5 min to an FiO2 of 0.15, by adding nitrogen into the chamber. Timings were recorded from when the FiO2 reached 0.15.
The criterion for a failed test was a need for supplemental oxygen as defined below:
For children with a baseline SpO2 of 95%–100%, the British Thoracic Society (BTS) guidelines6 were followed, and if desaturation occurred to 85%, oxygen was administered immediately to the child and titrated to reach the baseline SpO2 (nasal cannulae were already in place).
For those with a baseline SpO2 of 85%–94%, oxygen was administered if they desaturated by 15% of their baseline resting SpO2.
For those with a baseline SpO2 of 75%–84%, supplemental oxygen was given when SpO2 reached 70% as this was considered to be safe practice.
No child developed a significant cardiorespiratory deterioration during the test. The minimum amount of oxygen required to normalise saturation or to return to their abnormal baseline was documented. It was noted whether the child was awake (calm, active or unsettled/crying) or asleep. The parents were informed of the results immediately.
Statistical analysis
Descriptive statistics are presented as median and IQR. Comparisons between groups were tested using Mann-Whitney U tests for continuous data, and Fisher’s exact tests for categorical data (pass vs fail). Comparisons within groups (baseline vs test results) were analysed using Wilcoxon tests. Statistical analysis was performed using GraphPad Prism V.7 for Mac (GraphPad Software, La Jolla, California, USA). A P value of <0.01 was arbitrarily considered statistically significant to take into account multiple contrasts.
Results
There were 68 children studied, with mean age 3.3 years (range 10 weeks–14.5 years); 53% were boys. Full details of the children’s cardiac diagnoses and surgical procedures, with classification of whether there was an actual/potential R–L shunt, and their test results are in online supplementary table 1. Conditions included septal defects, valvar stenosis, coarctation, transposition of the great arteries, Ebstein’s anomaly, tetralogy of Fallot, truncus arteriosus and complex univentricular pathway cases such as variants of pulmonary atresia and atrial isomerism. Patients were also included among the various stages of total cavopulmonary connection (TCPC) pathway, for example, postmodified Blalock-Taussig shunt, postbidirectional cavopulmonary anastomosis and TCPC completion. One child was later diagnosed with a left vocal cord palsy and tracheobronchomalacia causing stridor, and another had mild tracheomalacia, but it was felt their results were unaffected (they both passed) so they were not retrospectively excluded from the study.
Supplemental material
Oxygen saturation
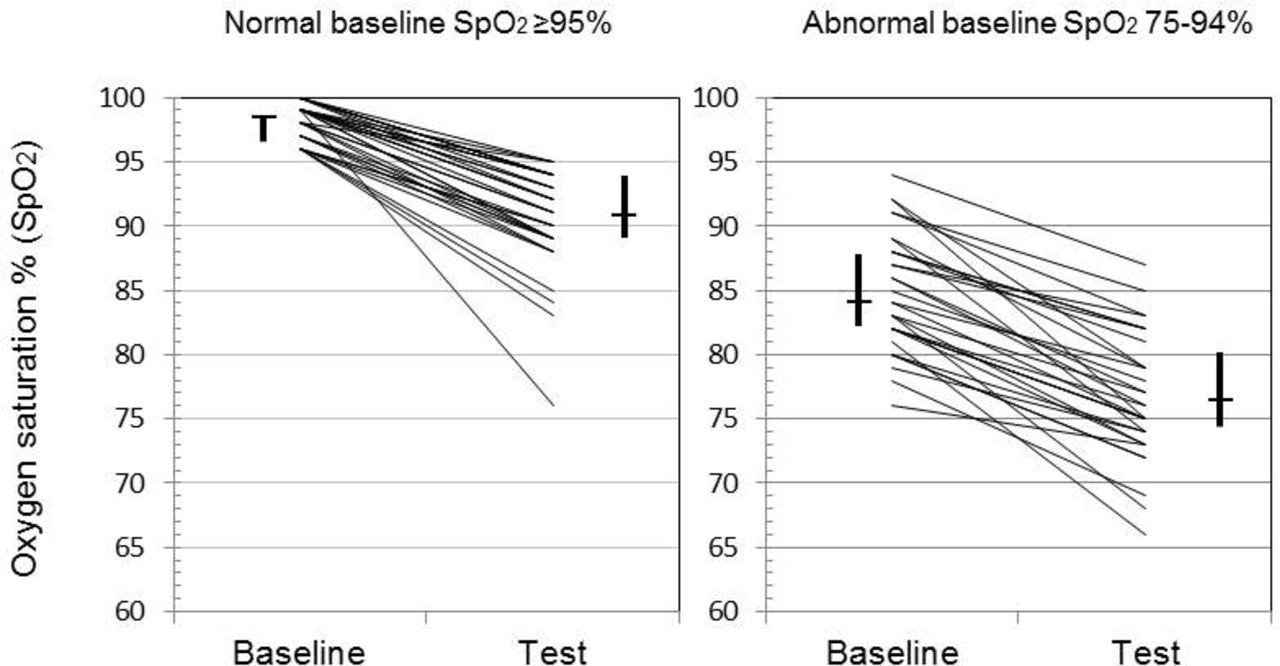
Normal versus abnormal baseline SpO2: baseline data and Hypoxic Challenge Testing results are in table 1 and figure 1. Both groups had a significant fall in SpO2 during the testing (P<0.0001). There were 3/38 (8%) children who failed with normal baseline SpO2, and 5/32 (16%) who failed with abnormal baseline SpO2 (P=0.46).
Actual/potential R–L shunt: baseline data and Hypoxic Challenge Testing results are in table 2 and figure 2. Both groups had a significant fall in SpO2 during the testing (P<0.0001). Those children with no R–L shunt (actual or potential) all passed the test (0/25 failed), whereas in those with an actual/potential R–L shunt (operated or unoperated) 8/43 (19%) failed (difference between groups P=0.02).
Pass versus fail: – baseline data and Hypoxic Challenge Testing results are in online supplementary table 2. Both groups had a significant fall in SpO2 during the testing with P<0.0001 for those who passed (n=60) and P<0.01 for those who failed (n=8). There were no differences in baseline data (age, SpO2, PtcCO2, heart rate or QTc) that could predict failing the test. All those who failed the test had an actual/potential R–L shunt, or had not undergone repair, or had undergone palliative surgery; comparing the 35 who passed versus the eight who failed within this group, there were no baseline differences that predicted failing. Supplemental O2 was given to patients who reached the cut-off, and 0.5 L/min returned their SpO2 to baseline or to a level that was above the failure cut-off (this excluded one patient who could not tolerate the nasal cannulae so he was put straight back into air when he failed the test). No child developed a significant cardiorespiratory deterioration during the test.
Baseline data and hypoxic challenge testing results for those with normal (≥95%) versus abnormal baseline (<95%) SpO2

Baseline and Hypoxic Challenge Testing SpO2 for those with normal baseline SpO2 of ≥95% (n=36) versus abnormal baseline SpO2 of 75%–94% (n=32). Also shown are medians (horizontal line) and IQRs (vertical lines). SpO2, arterial oxygen saturation measured by pulse oximetry.
Baseline data and Hypoxic Challenge Testing results for those with no actual/potential R–L shunt versus those with an actual/potential R–L shunt or unrepaired/palliated

{kind=link}
{kind=link}
Baseline and Hypoxic Challenge Testing SpO2 for those with no actual/potential R–L shunt (n=25) versus those with an actual/potential R–L shunt or unrepaired/palliated (n=43). Also shown are medians (horizontal line) and IQRs (vertical lines). R–L, right to left; SpO2, arterial oxygen saturation measured by pulse oximetry.
Transcutaneous CO2
At baseline was significantly lower in those with abnormal baseline SpO2 (P=0.002) and in those with an actual/potential R–L shunt (P<0.0001) (tables 1 and 2). Differences were maintained during the test in those with an actual/potential R–L shunt (P=0.0005) but was non-significant in those with abnormal baseline SpO2 (P=0.03). The PtcCO2 did not change significantly during the test indicating no child hyperventilated to compensate for hypoxic conditions; the maximum fall in PtcCO2 was 0.7 kPa in two children.
Heart rate
Was similar between all groups and did not change significantly during the test (tables 1 and 2).
QTc
Was measured in 59/68 children with a median (IQR) 409 ms (394–427) and range 348–481 ms. There was no significant change during the hypoxic conditions, although one 22-month-old girl did have an increase from an already long QTc of 481 ms to 507 ms. There were no significant differences between groups (tables 1 and 2).
SpHb
Was measured in 40/68 children (reliable results were not always possible due to technical limitations) with a median (IQR) 12.4 g/dL (11.3–13.0) and range 9.1–15.9 g/dL (tables 1 and 2). The SpHb was significantly higher in those with abnormal baseline SpO2 (P<0.001) and non-significantly higher in those with an actual/potential R–L shunt (P=0.02).
Activity states
During the test, only one child was feeding; 75% were calm; 13% active and 10% crying or unsettled; no child was asleep. The activity states during the test were similar to before the tests started. However, comparing those who passed versus those who failed during the test, there were more who were calm (80 vs 38%) and fewer who were active (12 vs 25%) or crying (7 vs 38%). Numbers are small, but combining active with crying, there was a greater proportion of active/crying babies in the fail group and a greater proportion of calm babies in the pass group (P<0.02).
Discussion
We carried out Hypoxic Challenge Testing in children with complex congenital heart disease to predict who was likely to desaturate significantly during airflight and thus which groups should have preflight testing. As expected, the SpO2 dropped in all children during the test but to variable degrees. The baseline SpO2 is unhelpful as a guide, since 3/36 (8%) failed with normal baseline SpO2 of 95% or above, compared with 5/32 (16%) with SpO2 <95%; although the proportion was twice as high in those with low SpO2, this difference was not significant. The underlying cardiac status was important, as no one failed the test unless they had an actual/potential R–L shunt, or who were unrepaired, or who had undergone palliative surgery, in which case 8/43 (19%) failed. Within the group who failed, there were no predictive factors found as to why they failed, compared with those with an actual/potential R–L shunt who passed. For this reason, our recommendation is to perform preflight Hypoxic Challenge Testing on all children with complex cardiac disease with an R–L shunt, as well as those with a potential to shunt (eg, TCPC patients with potential venovenous collaterals, Ebstein’s anomaly, common mixing conditions and obligate shunts), in order to determine who needs to have supplemental oxygen available for their flight. We are unable to make recommendations about airflight transfer of neonates or children in the emergency setting as we did not study this; however, those cases would likely travel with a medical escort and full monitoring anyway.
We excluded children with pulmonary hypertension, so we are unable to offer guidance for this group. However, the British Cardiovascular Society 2010 guidelines suggest passengers with established pulmonary vascular disease (Eisenmenger syndrome) should not be restricted from flying but should have supplemental oxygen8; a preflight Hypoxic Challenge Testing is therefore unnecessary as they are automatically going to have oxygen. Their advice is based on two small adult studies,9 10 including a UK survey of patients10; subsequently, there has been a survey on German adult patients with stable pulmonary hypertension that found 89% flew without significant complications.15 We did not test children with simple cardiac lesions, for examle, ventricular septal defect (VSD), atrial septal defect, patent ductus arteriosus, but could probably assume that if there is no actual/potential R–L shunt, they should be able to fly without extra oxygen and there is no need for preflight testing. It is important to know whether the children have associated pulmonary hypertension following results of a study that is over 30 years old, of 29 children with congenital heart disease and pulmonary hypertension.16 Twenty-two preoperative and 15 postoperative patients (including eight tested both pre and post) had cardiac catheterisation breathing room air followed by 15% oxygen (equivalent to inflight). Preoperatively, there were significant increases in pulmonary arterial pressure, decreases in pulmonary blood flow and increases in pulmonary vascular resistance. Worryingly within 2–4 min, two children under 12 months old (one with a VSD, the other with complete atrioventricular septal defect and both with moderate pulmonary hypertension) developed severe pulmonary vasoconstriction with extreme hypoxaemia considered to be life threatening. Neither of them could have been predicted from baseline haemodynamic status compared with the other children. Postoperatively, no children had a significant pulmonary Ivascular response to the hypoxia.
Although part of the response to hypobaric hypoxia includes a mild tachycardia,17 we found the heart rate did not change significantly in any of the groups. QTc was assessed as hypoxia prolongs cardiac repolarisation measured by QTc; for example, a small study of 11 healthy adults found that breathing 11% oxygen led to significant increases in QTc,18 and a study of nine mountaineers found significantly prolonged QTc when at high altitude (ranging 4400–7800 m).19 However, a study in 101 adults with significant respiratory disease having a Hypoxic Challenge Testing showed that the QTc did not change during the test.20 This was in keeping with our results that showed no significant change in QTc at 15% oxygen, apart from in one child with a repaired tetralogy of Fallot and right bundle branch block.
Hypoxic Challenge Testing only answers the question whether supplemental oxygen will be required during airflight; it cannot predict whether a person will have other health problems, induced by the noise, vibration, dry air, disrupted sleep, cramped conditions and general stresses of overcrowding and travel, which is why it is no longer called a ‘fitness to fly test’.21 Hypoxic Challenge Testing is the test recommended by the BTS.6 However, it is a limitation of our study that while the test has been validated in adults in a hypobaric chamber,22 this has not been done in children. Furthermore, nor has the test been validated by testing adults or children during actual flight compared with the preflight Hypoxic Challenge Testing prediction. Nevertheless, it has been studied in children with several respiratory conditions, for example, cystic fibrosis, and particularly ex-preterm infants with chronic lung disease.23–26 It is the best test we currently have available. While we used the BTS standards developed for respiratory patients with normal baseline SpO2, we had to adapt the Hypoxic Challenge Testing pass/fail criteria for those starting with abnormal SpO2. This was based on a consensus view of what was felt to be safe for the patients, although we accept to an extent they were arbitrary. If a Hypoxic Challenge Testing is not available, and flight is essential, then it is safest to recommend supplemental oxygen. The alternative preflight test uses a tight-fitting non-rebreathing face mask with a one-way valve; it has been studied extensively in Australia, but it is no longer thought to be valid for predicting what happens during flight,27 so we do not use it even though the equipment is more readily available. This is backed up by a study of 36 adults with precapillary pulmonary hypertension who had Hypoxic Challenge Testing using a 40% Venturi mask with nitrogen used to provide an FiO2 at the mouth of 0.15.28 Fourteen of the subjects had previously flown, but the Hypoxic Challenge Testing failed to predict correctly from the history of symptoms the subsequent test results in a number of subjects. A small study that included seven children with congenital heart disease also used a face mask Hypoxic Challenge Testing and found that they desaturated significantly more while walking at 3 or 5 km/hour than at rest, which may be relevant if the child is walking up and down the aisle in the plane.29 Obviously, it is not possible to test the effect of exercise during a Hypoxic Challenge Testing in our body plethysmograph, apart perhaps while doing isometric arm exercises.
In conclusion, this is the first study to provide evidence on which paediatric cardiologists can make evidence-based recommendations to families, and the study should help them decide which children with complex congenital heart disease should have a Hypoxic Challenge Testing to determine who needs supplemental oxygen. We recommend that all children who have an actual/potential R–L shunt, have not yet had a repair or have had palliative surgery only should be tested.
Key messages
What is already known on this subject?
Commercial airplanes fly with an equivalent cabin fraction of inspired oxygen of 0.15 leading to reduced oxygen saturation in passengers. To what extent this affects children with complex heart disease is unknown, so there is a poor evidence base for recommending who needs supplemental oxygen when flying.
What might this study add?
Children without a right-to-left (R–L) intracardiac shunt all passed the Hypoxia Challenge Testing, whereas 19% of those with an actual/potential R–L shunt (operated or unoperated) failed.
How might this impact on clinical practice?
We recommend that all children who have an actual/potential R–L shunt, have not yet had a repair or have had palliative surgery only should undergo a preflight Hypoxia Challenge Testing.
Acknowledgments
We wish to thank the parents and children for participating in the study. Thanks also to Cara Bossley, Derek Cramer, Anne Sharpe and the clinical physiologists in the Lung Function laboratory for advice with the hypoxia challenge testing. Thanks to Jan Till for advice over data on QT intervals. Finally, thanks to Mark Rosenthal and Andrew Turnbull for statistical advice.
References
Footnotes
NN and VLD contributed equally.
PEFD and IMB-L contributed equally.
Contributors IMB-L and PEFD conceived the study, and SW and NNN contributed to the protocol. NNN and VLD recruited the patients. NNN, VLD and LS supervised the testing. SW contributed in the overall supervision of the testing. RCF categorised all the patients. VLD, NNN and IMB-L wrote the paper with contributions from all authors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval was granted by the South West London Research Ethics Committee (10/H0801/54).
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this article was first published online, equal contributor statements for the first and last set of authors have been added.