Article Text

Statistics from Altmetric.com
- Patent foramen ovale (PFO)
- atrial septal defect (ASD)
- transthoracic echocardiography (TTE)
- transoesophageal echocardiography (TEE)
- CT imaging
- embryology
- CT scanning, echocardiography (three-dimensional)
- echocardiography (transoesophageal)
Adult patients with atrial septal defects (ASDs) have variable clinical presentations that can range from dyspnoea on exertion to cerebral vascular accidents from paradoxical embolism. Currently echocardiography is the mainstay in the diagnosis and follow-up of patients with ASDs. As CT technology advances and low radiation techniques improve, cardiac CT is becoming a desirable method to evaluate patients with ASDs when echocardiographic evaluation is limited.
Correct diagnosis and appropriate management of patients with patent foramen ovales (PFOs) and ASDs relies on an understanding of the embryologic development patterns that resulted in the malformation and associated anomalies. In this review, we illustrate the development of the interatrial septum and the foramen ovale. We discuss the diagnosis of PFOs and ASDs by echocardiography and highlight the incremental benefit of CT to further elucidate defect morphology, associated anomalies, and anatomy post-repair.
Development of the interatrial septum
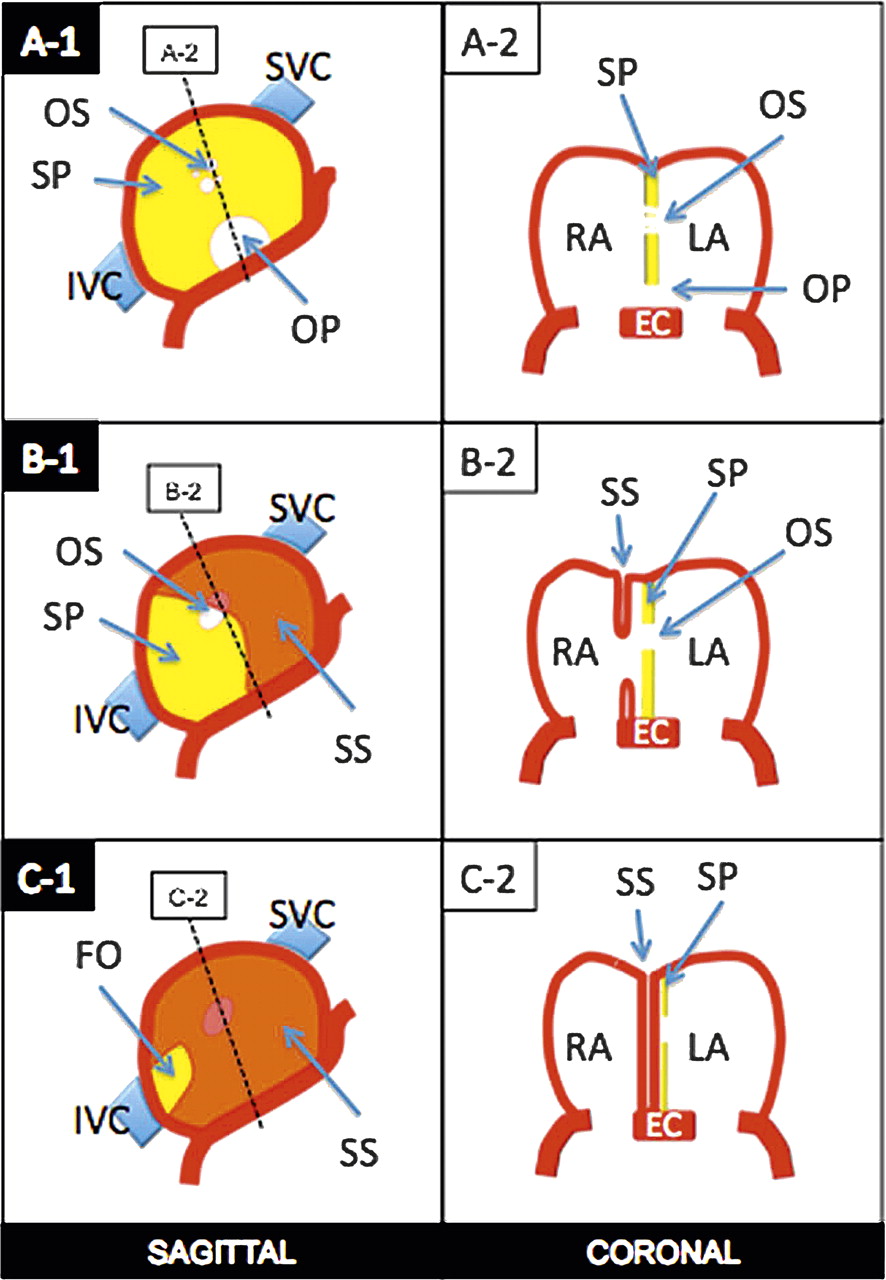
The primary atrium starts as a common cavity.1 Starting at 5 weeks of gestation, the primordial single atrium begins dividing into right and left sides by formation and fusion of two septa: the septum primum and septum secundum (figure 1). Early in the fifth week of gestation the septum primum begins to form near the centre of the roof of the common atrium, growing downward to the endocardial cushions, and partially dividing the common atrium into right and left counterparts (figure 1, A-1 and A-2). The gap between the septum primum and endocardial cushions is known as the ostium primum. Before the septum primum and endocardial cushions fuse, perforations develop within the cephalic portion of the septum primum through apoptosis, creating a large window known as the ostium secundum. At the end of the sixth week the caudal free edge of the septum primum reaches the atrioventricular cushions and fuses with them, closing the ostium primum (figure 1, B-1 and B-2).

Diagrammatic representation of the development of the interatrial septum. Beginning at the fifth week of gestation, the septum primum (SP) begins to develop and grows towards the endocardial cushions (EC). The gap between the EC and SP is known as the ostium primum (OP) (A-1 and A-2). Before the SP fuses with the EC, fenestrations develop in the cephalic portion of the SP creating a window called the ostium secundum (OS) (A-1 and A-2). Meanwhile, the septum secundum (SS) begins to form as an infolding of the ventrocranial atrial wall, to the right of the SP (B-1 and B-2). While the SS continues its caudal descent overlapping the OS, the OS fenestrations coalesce to form a larger fenestration (B-1 and B-2). The SS stops its growth leaving a small gap known as the fossa ovalis (FO) (C-1 and C-2). IVC, inferior vena cava; LA, left atrium; RA, right atrium; SVC, superior vena cava.
Towards the middle of the seventh week of gestation the septum secundum begins to develop. The septum secundum is a semilunar shaped infolding of the atrial roof which develops to the right of the septum primum. The septum secundum creates an incomplete separation of the atria, with a gap known as the fossa ovale (figure 1, C-1 and C-2). The floor of the fossa ovale is formed by the septum primum, which forms a flap valve mechanism.1 In utero, the inferior vena cava (IVC) flow is preferentially directed towards the interatrial septum, into the fossa ovale, between the layers of the septum secundum and septum primum and into the left atrium. This passage or ‘tunnel’ between the septum secundum and septum primum is the foramen ovale. Eventually, within the first 2 years of life, in most of the population the septum secundum fuses with the septum primum creating a complete physiologic and morphologic separation of the two atria and closing the foramen ovale (figure 2).2

Sagittal oblique image from a cardiac CT in a 66-year-old man demonstrates the septum secundum (SS) (orange), fossa ovalis (FO) and septum primum (dashed line). LA, left atrium; RA, right atrium; RPA, right pulmonary artery.
PFO: background and imaging
The lack of fusion between the septum primum and septum secundum results in a PFO. It is not considered a true ASD because there is no structural deficiency of atrial septal tissue. The foramen remains functionally closed as long as left atrial pressure is greater than right atrial pressure. Occasionally, under normal physiologic conditions, slightly higher pressures in the left atrium can translate into a left-to-right shunt.3 4 If right atrial pressure rises, the foramen ovale may open and there is potential for right-to-left shunting, the most devastating complication of which is stroke from paradoxical embolism.5 6
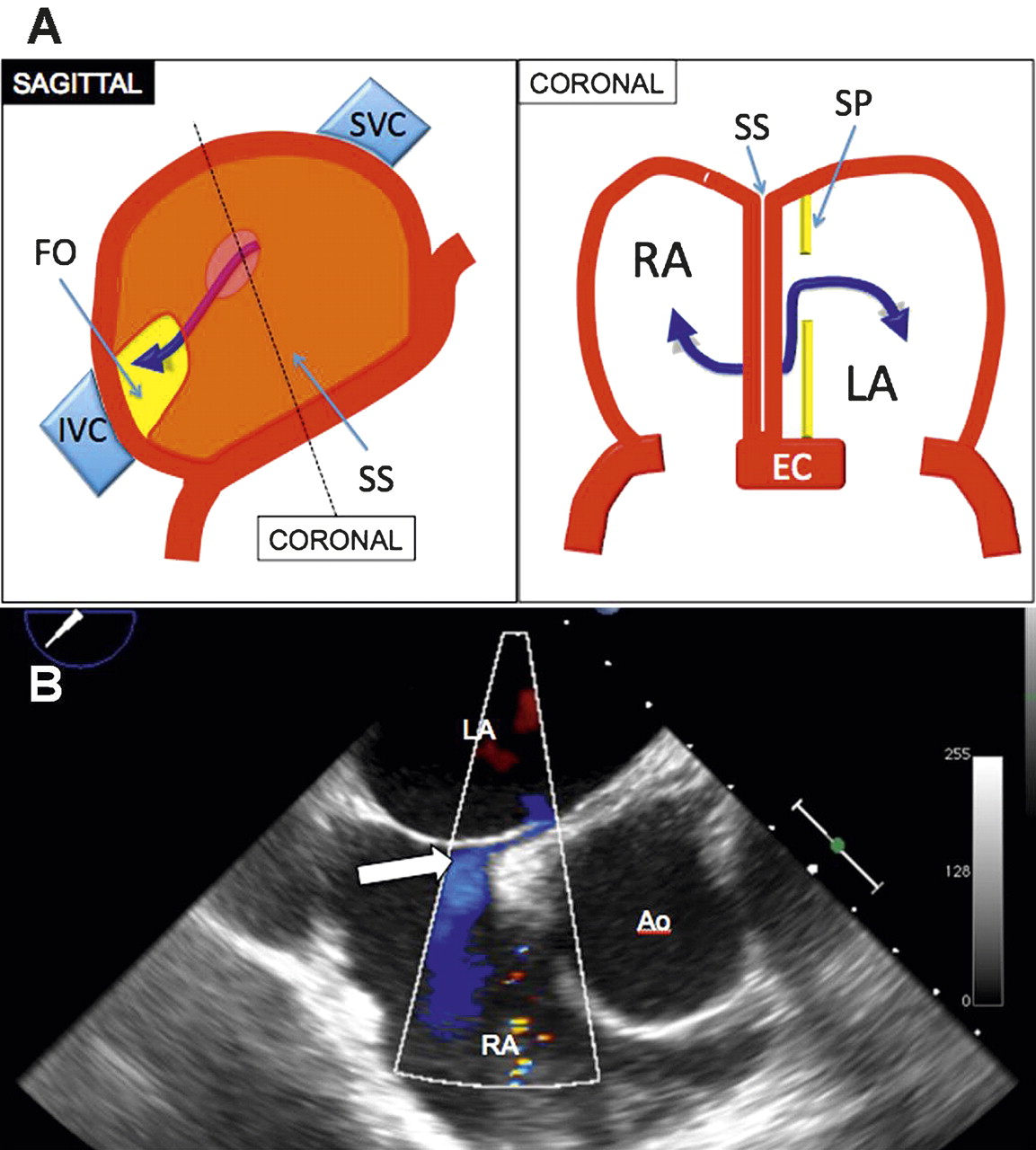
Transthoracic echocardiography (TTE) is commonly the first imaging modality used to assess PFOs. Venous injection of 5–10 ml of agitated saline at rest may reveal the passage of bubbles from the right atrium into the left atrium, suggesting right-to-left shunting (figure 3). The diagnosis of a PFO by contrast TTE depends on the identification of bubbles in the left atrium within three cardiac cycles. After more than three cardiac cycles, bubbles in the left atrium may reflect the transpulmonary and not transseptal passage of agitated saline bubbles.7 The degree of shunting and the size of the PFO can also be estimated via the number of bubbles that cross into the left atrium.

(A) Diagrammatic representation of a patent foramen ovale (PFO). The interatrial communication (double head arrows) occurs because of the lack of fusion between the septum secundum (SS) and the septum primum (SP). It is not considered a true atrial septal defect because there is no absent tissue. Note the normal appearance of the SS and SP. (B) Transoesophageal echocardiogram of the interatrial septum in an anteroposterior view. Colour flow imaging confirms the presence of a left-to-right shunt through a ‘tunnel’ consistent with a PFO (arrow). Ao, aorta; EC, endocardial cushions; FO, fossa ovalis; IVC, inferior vena cava; LA, left atrium; RA, right atrium; SVC, superior vena cava.
If the initial ‘bubble study’ is negative at rest, a comprehensive assessment for PFO would involve a repeat agitated saline injection during the Valsalva manoeuvre to determine whether a transient increase in right sided pressure above left sided pressure opens a PFO that was otherwise functionally closed. This manoeuvre is typically performed by asking the patient to attempt to exhale with moderate force while keeping the mouth and nose closed. As the right atrium begins to opacify following venous injection of agitated saline, the patient is asked to release the Valsalva strain.8 Similar to coughing, this transiently results in higher right sided pressures leading to the passage of bubbles from the right atrium into the left, thus aiding in the detection of a PFO during echocardiography.9 10 Colour Doppler by transoesophageal echocardiography (TOE) may also confirm the presence of a PFO by demonstrating interatrial shunting through a PFO (figure 3B).
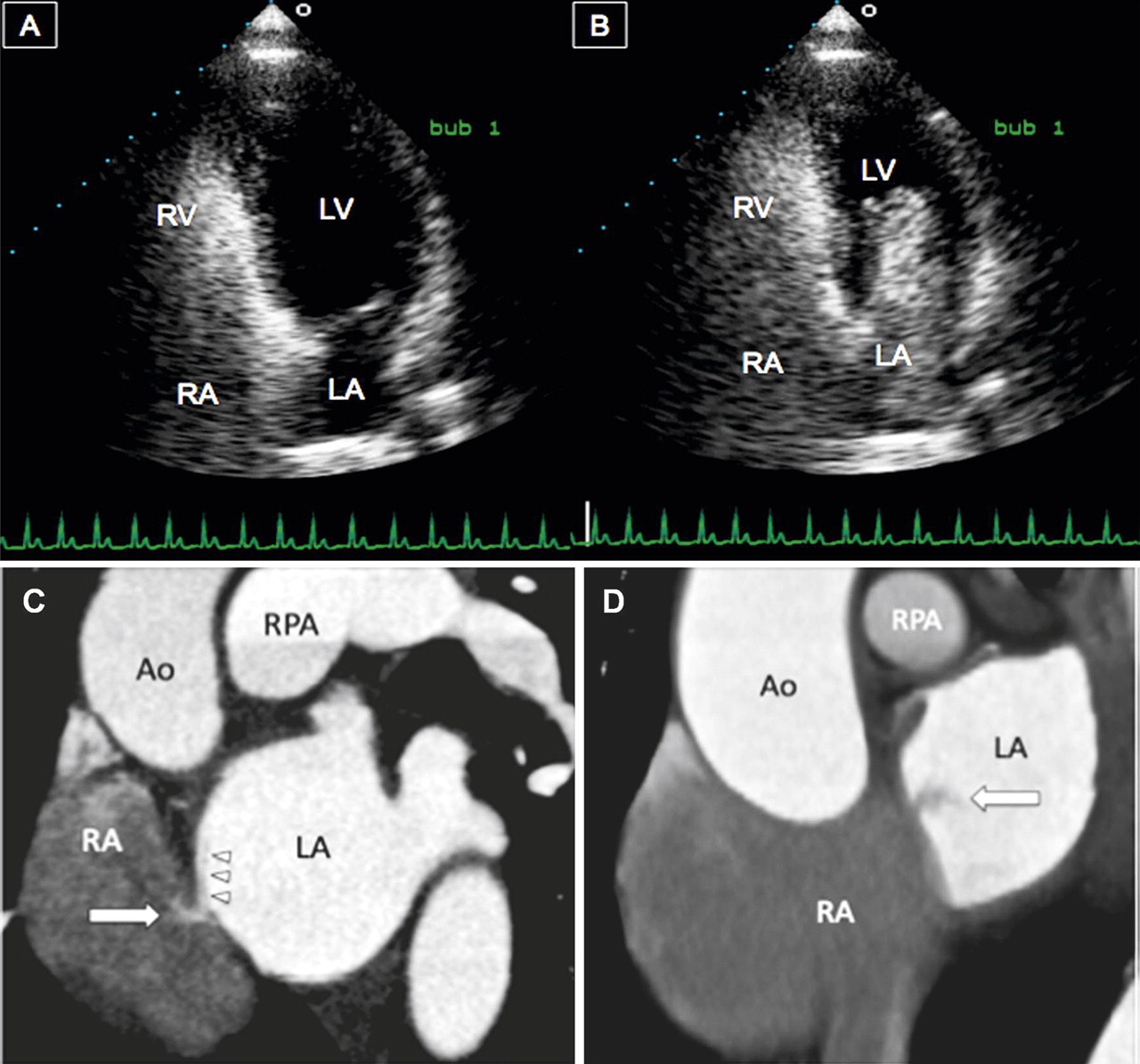
CT has also been used to diagnose a PFO. On multiphase short axis reconstructions, the left-to-right shunt of a PFO is seen as a high attenuation jet that projects towards the floor of the right atrium most prominently during mid diastole (50–70% of the R-R interval) (figure 4C).5 Conversely, in right-to-left shunts the jet may project towards the roof of the left atrium (figure 4D).

Apical four chamber views (A and B) from a transthoracic echocardiogram, acquired during a Valsalva manoeuvre in a 54-year-old woman with a stroke, demonstrate rapid opacification of the left chambers due to the presence of a patent foramen ovale (PFO). (C) Sagittal oblique image from a cardiac CT in a 43-year-old man with chest pain incidentally demonstrates the presence of a small jet of contrast extending from the left atrium (LA) into the right atrium (RA) consistent with a PFO. Note the presence of the flap valve of the septum primum (arrowheads) creating a tunnel. (D) Sagittal oblique image from a cardiac CT in a 57-year-old man with chest pain (right image) incidentally demonstrates a low density jet extending from the RA into the LA consistent with a PFO. Ao, aorta; LV, left ventricle; RPA, right pulmonary artery; RV, right ventricle.
ASDs: background and imaging
There are four types of ASDs, two of which can be morphologically classified as defects within the interatrial septum (ostium primum and secundum ASDs). The two other defects, sinus venosus and coronary sinus subtypes, physiologically behave as interatrial septal defects but do not involve a developmental abnormality of the interatrial septum per se.11
Similar to imaging of PFOs, echocardiography is the primary modality for the diagnosis, morphologic assessment, and follow-up of patients with ASDs. Nonetheless, the role of CT continues to grow, and although currently most ASDs identified on cardiac CT are detected incidentally, CT is an additional tool to assess morphology and associated anomalies when echocardiography is limited. Imaging of ASDs by CT requires adequate intracardiac opacification. In general, contrast material is administered using a biphasic protocol consisting of an initial contrast bolus at a rate of 4–7 ml/s, followed by 40–50 ml of saline, to flush out the contrast from the right heart. This method provides an ideal opacification of the left heart for the detection of left-to-right shunts. Using this same technique, right-to-left shunts (mainly seen in PFO or large ASDs with Eisenmenger physiology) can be seen as low attenuation jets entering the opacified left atrium.
The mode of data acquisition, whether prospective or retrospective, is a significant topic. Retrospectively gated acquisition uses helical scanning, exposing the patient to radiation during the entire cardiac cycle. On the other hand, prospective gated acquisition obtains information during a specific point in time, significantly reducing radiation exposure. Given that intracardiac shunting in patients with ASDs commonly occurs in late diastole (70% R-R interval), prospective gating is preferred whenever feasible (with a regular, slow heart rate).
As an aside, the use of cardiac magnetic resonance and phase contrast imaging allows for the precise quantification of intracardiac shunting and morphologic assessment of ASDs. This imaging modality should be used instead of CT when the severity of intracardiac shunting is in question. However, the higher spatial resolution of cardiac CT allows better assessment of the morphology of these defects and their associated anomalies.
As the various types of ASDs are associated with distinctive clinical presentations in different areas of the heart, it is important to select effective imaging modalities permitting a comprehensive diagnosis and morphological assessment. Therefore, we briefly highlight the contributing developmental processes for each of the four types of ASDs along with their respective clinical presentations in the context of medical imaging.
Ostium primum ASD
An ostium primum ASD results from the lack of fusion between the septum primum and the endocardial cushions (figure 5A). Ostium primum septal defects, which correspond to 2–3% of all ASDs, represent a mild form of atrioventricular septal defects or endocardial cushion defects which are commonly associated with trisomy 21.12 In normal development, the endocardial cushions contribute to the formation of the medial portions of the atrioventricular valves, the portion of the atrial septum adjacent to the atrioventricular valves, and the inlet portion of the ventricular septum. When the defect is isolated, due to failure of fusion between the free edge of the septum primum and the atrioventricular cushions, it is termed an ostium primum ASD (figure 5B). If this defect is associated with abnormal development of the atrioventricular valves or ventricular septum it is known as an atrioventricular septal defect or endocardial cushion defect.11

(A) Diagrammatic representation of an ostium primum atrial septal defect (ASD). Incomplete fusion between the developing septum and the endocardial cushions (EC) results in an abnormal communication between the two atria (double head arrows) adjacent to the atrioventricular valves. (B) Apical four chamber view from a transthoracic echocardiogram from a 38-year-old patient with dyspnoea on exertion demonstrates an interatrial communication (curved arrow) located immediately behind the insertion of the atrioventricular valves (arrowheads) consistent with an ostium primum ASD. Note the enlargement of the right sided chambers due to volume overload from left-to-right shunting. FO, fossa ovalis; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; SP, septum primum; SS, septum secundum; SVC, superior vena cava.
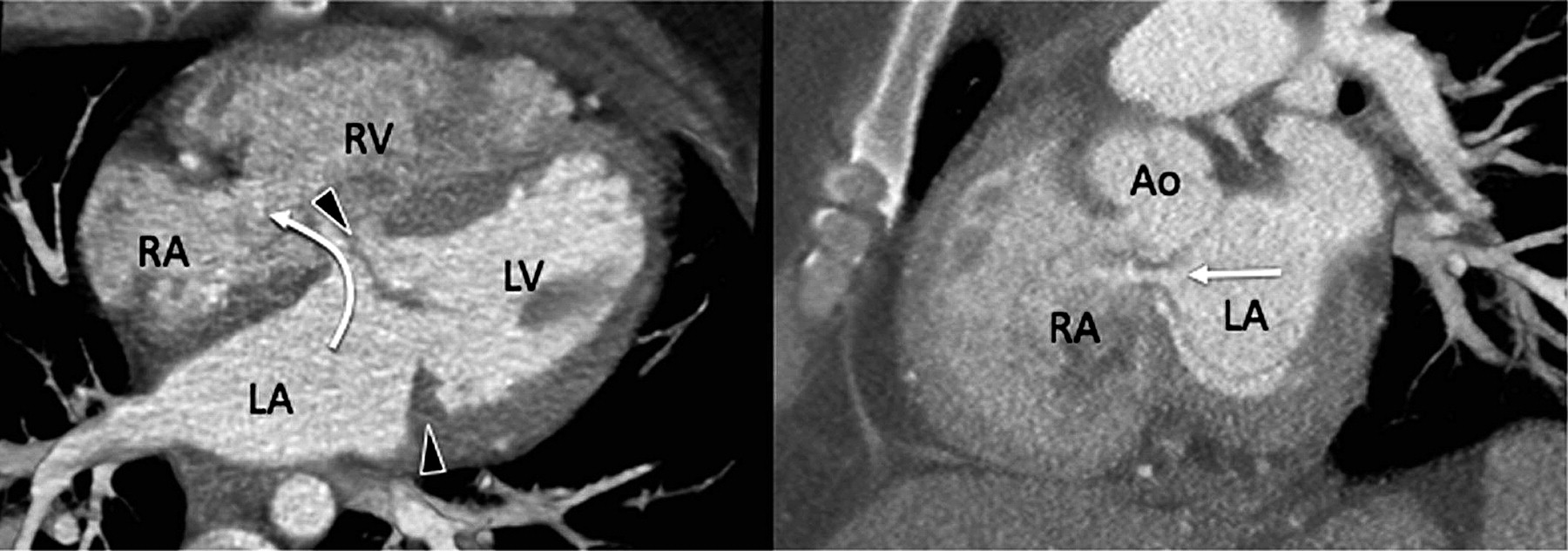
On cardiac CT, ostium primum ASDs can be seen as an abnormal communication between the right and left atria located immediately posterior to the mitral valve annulus (figure 6). Depending on the size of the defect, relative equalisation of contrast density in the right and left chambers can be seen. Additionally, there is usually associated enlargement of the right sided chambers.

Four chamber (image on the left) and short axis (image on the right) views from a cardiac CT in a 23-year-old man with dyspnoea on exertion demonstrate the presence of a small ostium primum atrial septal defect (curved and straight arrows). Note the location of the atrial septal defect immediately behind the insertion of the mitral valve (arrowheads). Ao, aorta; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
Ostium secundum ASD
Ostium secundum ASDs result from excessive apoptosis of the cephalic portion of the septum primum or incomplete development of the septum secundum (figure 7A). Ostium secundum ASDs comprise 80–90% of ASDs and are located along the fossa ovalis of the interatrial septum.

(A) Diagrammatic representation of an ostium secundum atrial septum defect (ASD). Abnormal development of the septum secundum (SS) and/or septum primum (SP) results in a direct communication of the two atria (doublehead arrows) in the region of the fossa ovalis (FO). (B) Four chamber image from a cardiac CT in a 23-year-old woman demonstrates a large defect in the mid interatrial septum (arrow) consistent with an ostium secundum ASD. Note the enlargement of the right atrium (RA), right ventricle (RV) and right pulmonary artery (RPA) due to longstanding volume overload. Also note the relative equalisation of contrast density among the left and right cardiac chambers due to free mixing of contrast. EC, endocardial cushions; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; SVC, superior vena cava.
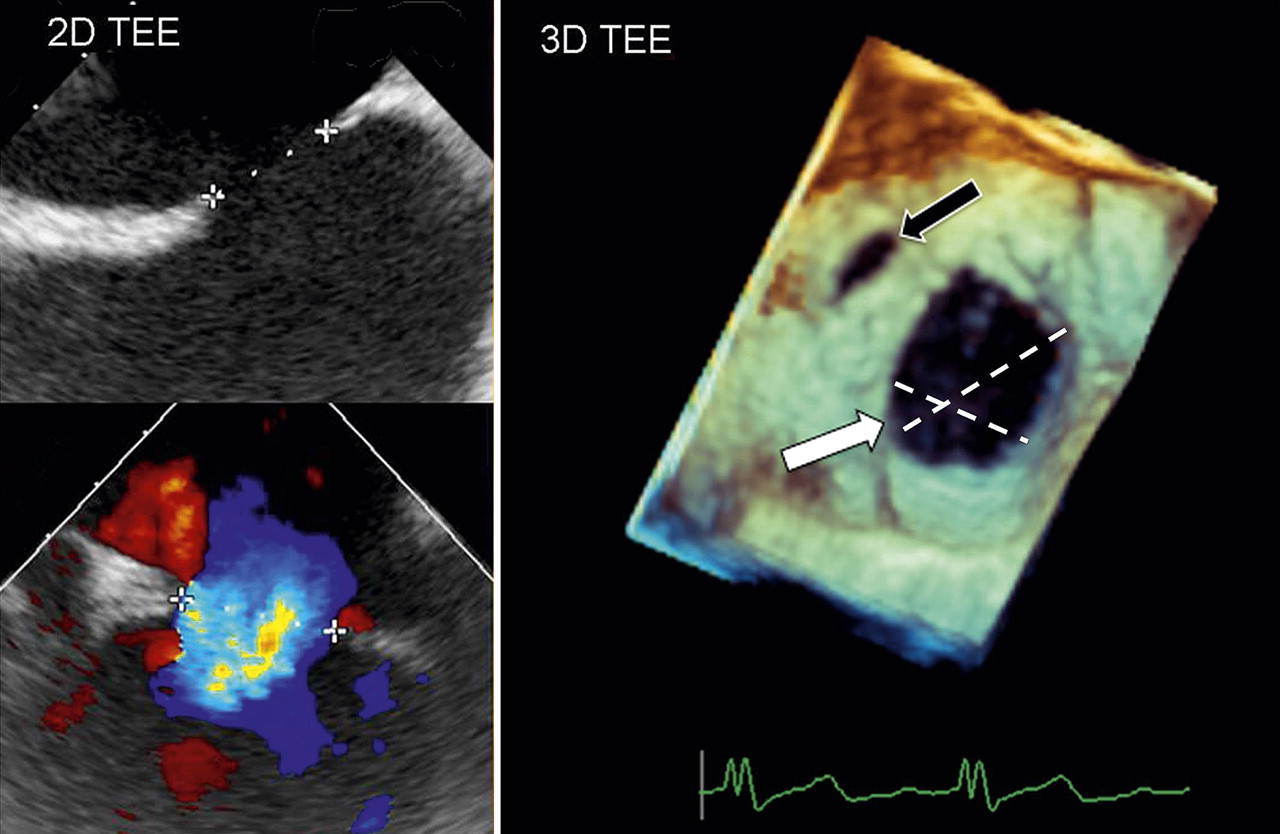
Echocardiographically, ostium secundum ASDs are typically found in the central portion of the interatrial septum and can be multiple or associated with fenestrations. Occasionally, if a patient presents with poor acoustic windows, the cause of right atrial and right ventricular enlargement may not be readily apparent using TTE. In such situations, TOE may help to define better the presence of one or more defects, as well as accurately size the defect before repair. ASD shape and size can vary significantly, and may be elliptical, complex (irregularly shaped), or circular. Thus imaging the septum from several planes is crucial. Nonetheless, two dimensional (2D) TOE can underestimate the area of complex shaped ASDs. Therefore, real-time three dimensional (3D) echocardiography can be used to delineate the size, shape and number of defects better, and is particularly relevant for irregular and complex shaped ASDs (figure 8).13 14

Two dimensional (2D) transoesophageal echocardiographic and contrast images show only one plane of the atrial defect. To measure the size and shape of the defect accurately, multiple 2D image acquisitions are required to form a mental image of the defect's three dimensional (3D) structure. Note that additional minor secundum defects may be missed using 2D transoesophageal echocardiography. In the right panel, 3D transoesophageal echocardiography image of the interatrial septum enface clearly demonstrates the presence of two secundum defects (black and white arrows). From this dataset, multiplanar reconstructions allow for measurement of the long axis of each defect and the area of each defect. In this particular case, the size and number of defects precluded transcatheter device closure.
On cardiac CT, ostium secundum ASDs are seen as defects of variable size in the region of the fossa ovalis (figure 7B). Differentiating a PFO and small ostium secundum ASD can be difficult, but in general the tunnel of a PFO will direct flow to the roof of the left atrium or to the floor of the right atrium, in contrast to the flow of ostium secundum ASDs which tend to be horizontal. CT can also help to assess the morphology of the ASD, adequacy of rim size, and associated enlargement of the right side chambers and pulmonary arteries.
Sinus venosus ASD
Sinus venosus defects are thought to occur due to malpositioning of the insertion of the superior vena cava (SVC) or IVC into the right atrium or deficiency of the wall that separates the right sided pulmonary veins from the SVC or right atrium, creating a communication between the two atria.15 Sinus venosus ASDs are located between the venous inflow of either the SVC or the IVC and the left atrium.
The superior sinus venosus defect (SSVD) accounts for 2–3% of all interatrial communications. It is located at the superior cavo–atrial junction and is frequently associated with anomalous drainage of the right sided pulmonary veins into the SVC or right atrium.16 17
SSVDs can be difficult to detect using TTE due to their location in the far field of view. On the other hand, TOE is well suited to detecting an SSVD due to the closer proximity of the transducer to the defect. An SSVD can be identified using TOE by the absence of the atrial septum immediately beneath the orifice of the SVC.18 The challenges associated with echocardiography to detect commonly associated anomalies in the pulmonary venous return makes CT a reasonable alternative for evaluation of these patients.
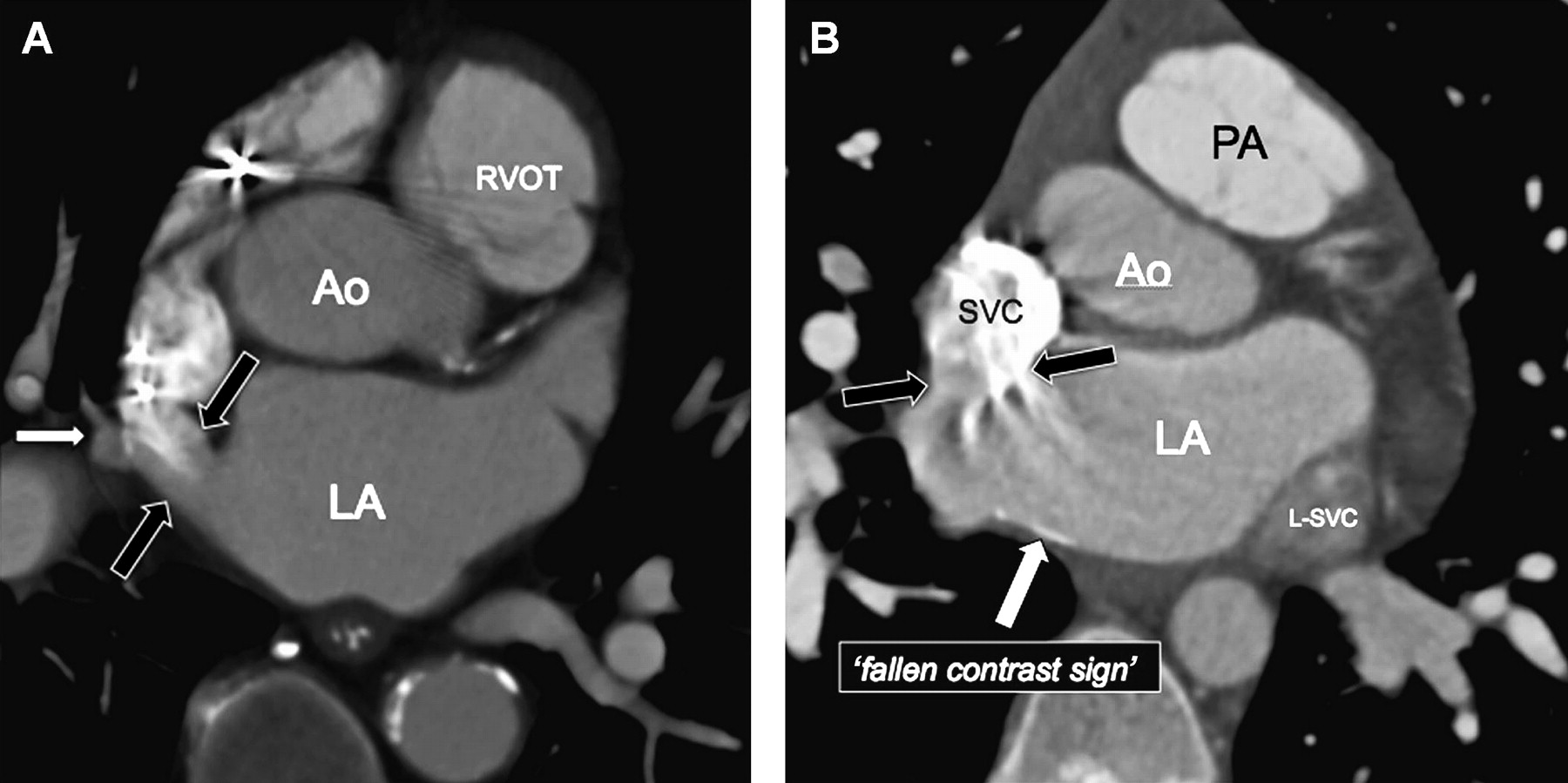
CT with intravenous contrast can demonstrate the defect as a communication between the SVC–right atrial junction and the left atrium (figure 9A). Due to the abnormal communication between the SVC–right atrial junction and the left atrium, another clue to the diagnosis is visualisation of concentrated contrast material accumulating in the posterior wall of the left atrium, which is known as the ‘fallen contrast sign’ (figure 9B). CT is excellent for detecting the presence of partial anomalous pulmonary venous return (PAPVR), which is commonly associated with SSVD but cannot be easily visualised by echocardiography.

(A) Axial image from a cardiac CT in a 75-year-old man, with biventricular heart failure s/p placement of a pacer/defibrillator, demonstrates a communication between the left atrium (LA) and the superior vena cava (SVC)–right atrial junction (black arrows) consistent with superior sinus venosus atrial septal defect (ASD). Also note the presence of anomalous pulmonary venous return into the sinus venosus defect (white arrow). (B) Axial image from a cardiac CT in a 45-year-old man with exertional dyspnoea demonstrates a sinus venosus ASD (black arrows). Due to the higher density of the contrast material relative to blood, contrast is noted pooling in the dependent portion of the left atrium consistent with the ‘fallen contrast sign’. Also present is a large vascular structure adjacent to the lateral aspect of the left atrium consistent with a persistent left SVC (L-SVC) which drained into the coronary sinus (not shown). Ao, aorta; PA, pulmonary artery; RVOT, right ventricular outflow tract; s/p, status post.
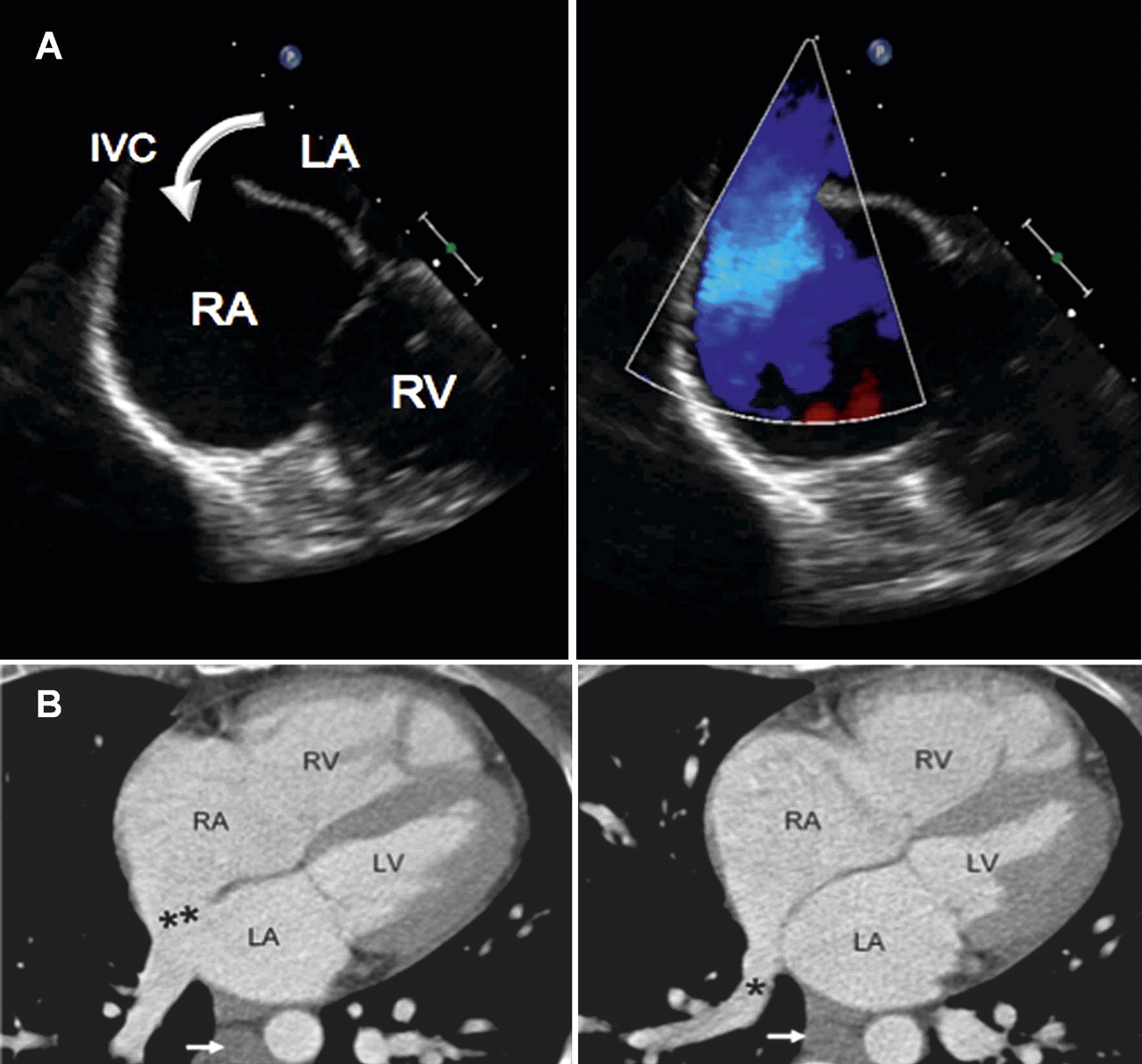
An inferior sinus venosus defect (ISVD) is located at the junction of the IVC and right atrium. It may be associated with anomalous drainage of a right inferior pulmonary vein into the intrapericardial segment of the IVC or right atrium. Using TOE and CT, an ISVD can be identified as a lack of tissue normally present between the IVC and the right atrium (figure 10A,B).19 In addition, colour flow imaging can further identify an ISVD defect through the presentation of left-to-right shunting from the pulmonary vein to the right atrium.

(A) Transoesophageal echocardiogram in a 38-year-old patient with an inferior sinus venosus defect. Image on the left demonstrates the defect at the junction of the inferior vena cava (IVC) with the right atrium (RA) (curved arrow). The defect measured 26 mm in the superior–inferior dimension. Image on the right with colour flow imaging indicates left-to-right shunting. Associated right atrial dilatation is also noted. (B) Four chamber views of an ECG gated cardiac multidetector CT from a 44-year-old woman with exertional dyspnoea demonstrate a large defect (double asterisk) in the inferior and posterior interatrial septum near the IVC–RA junction consistent with an inferior sinus venosus atrial septal defect (left image). There is associated abnormal right lower lobe pulmonary venous return into the right atrium (asterisk) (right image). Also noted is an enlarged azygos vein secondary to azygos continuation of the IVC (white arrow). LA, left atrium; LV, left ventricle; RV, right ventricle.
Unroofed coronary sinus
Coronary sinus ASDs are exceedingly uncommon. They occur when there is lack of septation between the back wall of the left atrium and the coronary sinus due to abnormal cell death during embryologic development, resulting in abnormal drainage of venous blood into the left atrium. The ‘unroofed’ portion of the coronary sinus connects to the inferior aspect of the left atrium before draining into the right atrium. Often associated is a persistent left SVC due to failure of degeneration of the left anterior cardinal vein.20
An unroofed coronary sinus defect on TTE may appear as a left-to-right shunt from the left atrium into a dilated coronary sinus in the parasternal long axis view (figure 11). In addition to dilatation of the left atrium and coronary sinus, any associated right atrial and right ventricular dilatation should also be assessed by TTE. The presence of a persistent left SVC can be determined by TTE or TOE after injection of agitated saline into the patient's left antecubital vein and assessing for the presence of saline bubbles in the coronary sinus before appearance in the right heart.

Parasternal long axis view from a transthoracic echocardiogram demonstrates an enlarged coronary sinus (CS) and left atrium (LA) with an obvious communication between the two structures due to a defect in the back wall of the CS (arrow) (left image). The use of colour flow imaging confirms shunting from the LA into the dilated CS (right image). Ao, aorta; LV, left ventricle.
Cardiac CT images of an unroofed coronary sinus defect typically reveal low attenuation of the coronary sinus upstream from the defect and equalisation with the enhanced left atrium at the level of the defect. This equalisation is due to free communication between these two structures, as well as shunting of high attenuation blood downstream into the right atrium (figure 12).

Coronal oblique, ECG gated cardiac multidetector CT (MDCT) image (left image) demonstrates lack of septation between the left atrium (LA) and coronary sinus (CS) roof (arrows) consistent with an unroofed CS. Note the poor opacification of the CS upstream from the defect with equalisation relative to the LA at the unroofed portion of the CS. Coronal oblique ECG gated cardiac MDCT image of a different patient (right image) for comparison demonstrates normal septation and fat plane (arrowheads) dividing the CS and the LA. Note the substantially lower opacification throughout the CS compared to the LA. Ao, aorta; LVOT; left ventricular outflow tract; RA, right atrium; RVOT, right ventricular outflow tract.
Imaging of ASD/PFO repair
The management of an adult patient with an ASD depends upon a number of factors including symptoms, the size and morphology of the defect, the presence of right ventricular dilation and/or pulmonary hypertension.21 Patients with ASDs and significant left-to-right shunting (>1.5:1) usually have associated right ventricular volume overload and require closure to prevent long term complications such as atrial and ventricular arrhythmias, reduced exercise tolerance, and right heart failure.22
The management of patients with a PFO is still controversial. The risk of stroke associated with an incidentally discovered PFO, ASD, and/or atrial septal aneurysm in asymptomatic individuals is uncertain. The role of primary prevention in this setting has not been established. For secondary prevention of stroke in this setting, medical treatment with aspirin or coumadin is recommended.
Percutaneous PFO closure received humanitarian device exemption approval from the US Food and Drug Administration (FDA) in 2001 in patients with recurrent cryptogenic stroke due to presumed paradoxical embolism that occurred despite appropriate anticoagulation. However, because of the lack of randomised clinical trial evidence supporting long term safety of percutaneous PFO closure devices and their efficacy in preventing stroke, humanitarian device exemption approval was withdrawn in 2006. Moreover, a significant increase in percutaneous PFO closures may have impeded enrolment targets in clinical trials aimed at characterising the effectiveness and safety of the devices and procedures.23 As percutaneous ASD closure devices remain available and in use, many physicians convinced of their safety and effectiveness in PFO closure continue to perform off-label procedures with ASD closure devices to block interatrial communication and reduce the risk of further strokes. Although uncertainty regarding the best approach to treat recurrent stroke in the setting of PFOs remains, most ostium secundum ASDs and PFOs can be closed via the minimally invasive percutaneous catheter technique (figure 13).

Three dimensional echocardiographic view of the interatrial septum enface from the left atrium (LA) by real time demonstrates an ostium secundum atrial septal defect (black arrow) through which an Amplatzer occluder device (white arrow) has been deployed. The left atrial disc of the device is seen in this view just before engagement with the interatrial septum. Image on the right shows a two dimensional transoesophageal echocardiogram of the device after deployment and assessment of residual shunt by colour flow imaging. Both the right atrial and left atrial discs of the device have been released and deployed across the defect. The device (white arrows) is seen from its side in the bicaval view. There is no evidence of residual shunt by colour flow imaging and the device appears well seated. RA, right atrium.
Two and three dimensional TOE are important modalities used to select defects for closure and guide placement before final release of the device.13 Before an ASD or PFO closure is attempted, a comprehensive evaluation of the defect is required to determine size, shape, and relationship to surrounding structures.2 Not all defects are anatomically suitable for transcatheter closure as a sufficient rim of interatrial septal tissue (4 mm in each direction) between the defect and adjacent structures is required to seat the device.14
Following deployment, TOE helps to rule out impingement of the device upon valves, veins, and the outflow tract and is used to assess the degree of residual shunt (figure 14). TTE is performed within 24 h after device closure and periodically following the procedure to assess for device position and residual shunt with the use of colour flow imaging and agitated saline contrast. Once appropriately selected for device closure, patients undergoing the transcatheter technique have excellent early and intermediate term follow-up results.

Two dimensional transoesophageal echocardiogram (TOE) from a 24-year-old woman during secundum atrial septal defect closure using an Amplatzer device. The device has been engaged along the interatrial septum and TOE allows for visualisation of placement before release. In this anteroposterior view both the right atrial and left atrial discs of the device (arrows) appear to adequately engage the interatrial septum before device release. LA, left atrium; IVC, inferior vena cava; RA, right atrium; SVC, superior vena cava.
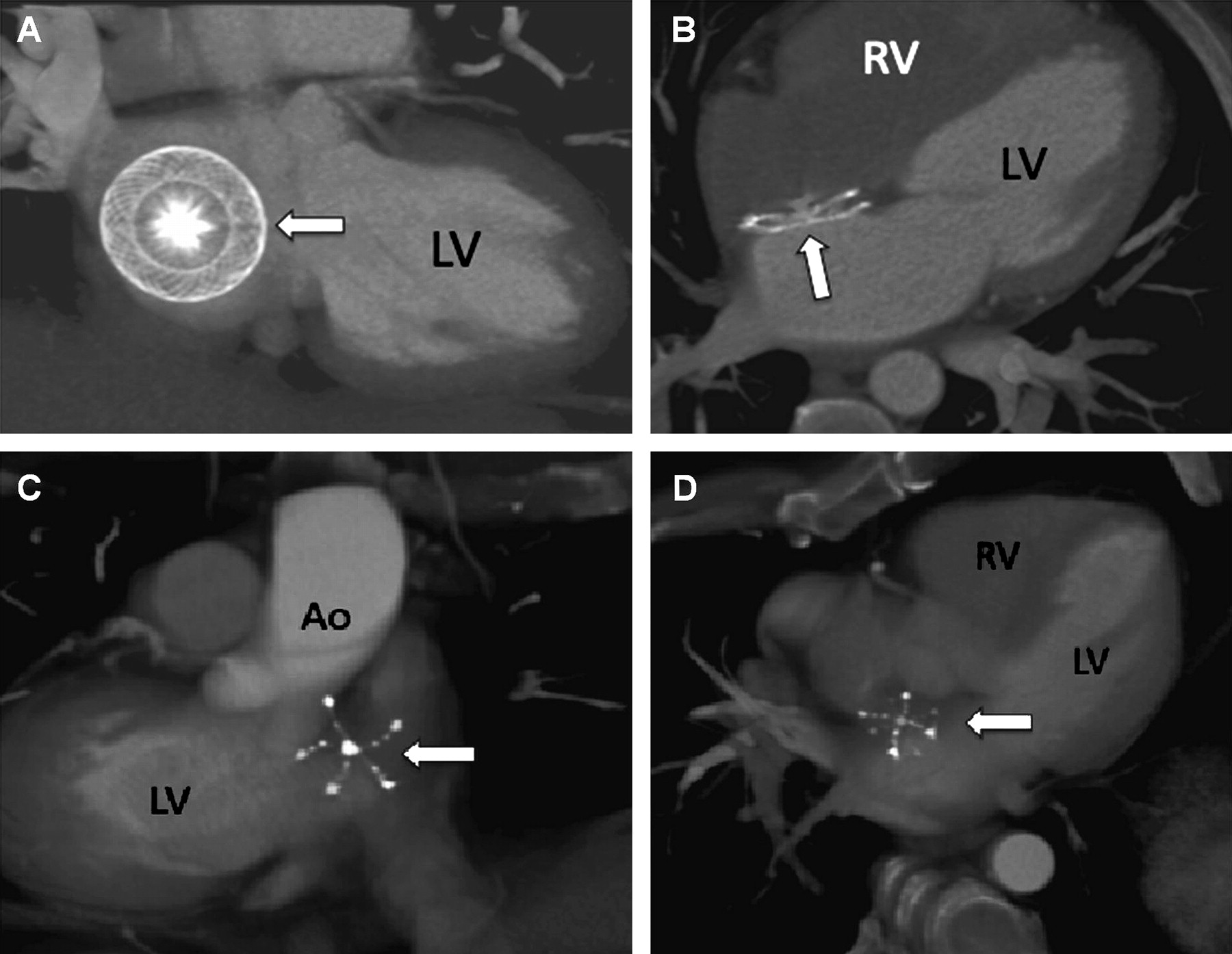
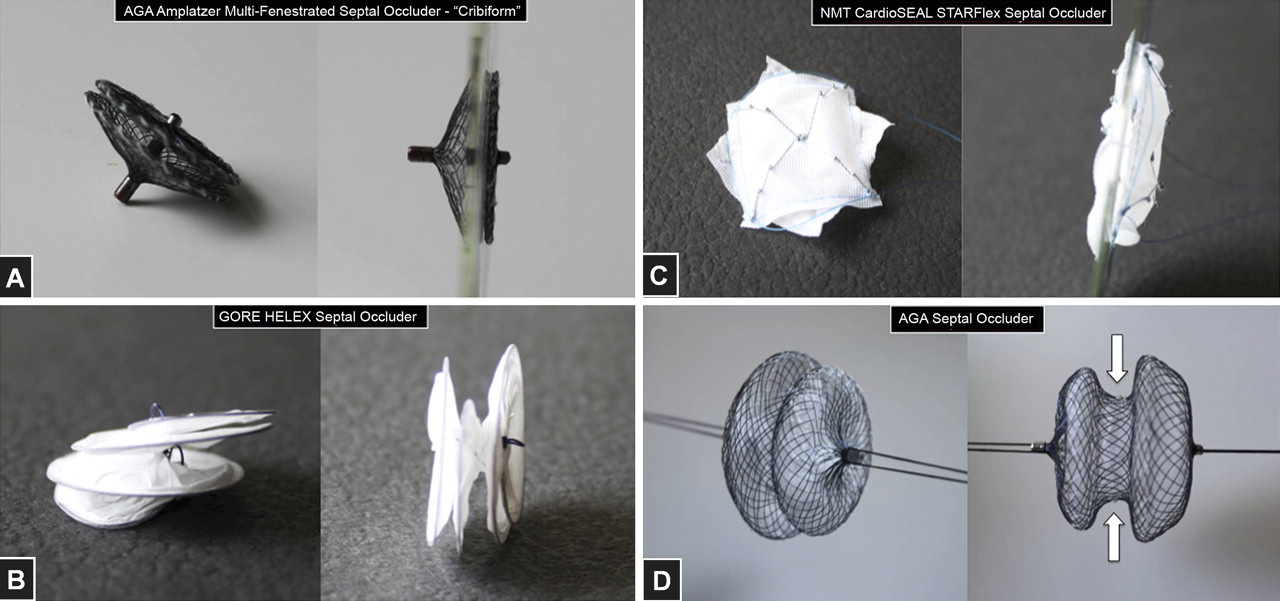
Both cardiac CT and 3D TOE now provide excellent detail of the closure devices following deployment; thus familiarisation with the various brands facilitates assessment of device position and seating (figure 15). There are two types of interatrial communication closure devices, the ‘non-self centred devices’ or single pin device, and the waist or ‘self centred devices’ (figure 16). Among the family of single pin devices, there are two different brands: the AGA Amplatzer multi-fenestrated septal occluder—‘Cribiform’ (AGA, Plymouth, Minnesota, USA), and the Gore Helex septal occluder (GL Gore & Associates, Flagstaff, Arizona, USA). These devices are approved for the closure of small ASDs, but are widely and mainly used as an off-label indication for PFO closure. The ‘self centred devices’ have a ‘waist’ that connects the right and left atrial disk. There are two self centred devices available in the USA to close ASDs: the AGA Amplatzer septal occluder (AGA) and the NMT CardioSeal StarFlex septal occluder (NMT Medical, Boston, Massachusetts, USA). The AGA muscular occluder is a self centred device used to close ventricular septal defects. The AGA Amplatzer septal occluder is characterised by a 4 mm larger left atrial disk diameter compared to the right atrial disk diameter.

(A, B) Paraseptal (left) and four chamber (right) images from a cardiac CT in a 26-year-old woman after closure of a large ostium secundum atrial septal defect (ASD) with an AGA septal occluder (white arrow). (C, D) Paraseptal (left) and four chamber (right) volume rendered images from a cardiac CT in a 39-year-old man after closure of a small ostium secundum ASD with a CardioSeal StarFlex septal occluder device (white arrows). Ao, aorta; LV, left ventricle; RV, right ventricle.

‘Non-self centred devices’ such as (A) the AGA Amplatzer Cribiform and (B) the Gore Helex septal occluder are used for small atrial septal defect (ASD)/patent foramen oval closure. (C) NMT CardioSeal StarFlex and (D) AGA septal occluders are ‘self centred devices’ used for ASD closure. Notice the ‘waist’ (arrows) that connects the right and left atrial disk and the difference in size between the two disks.
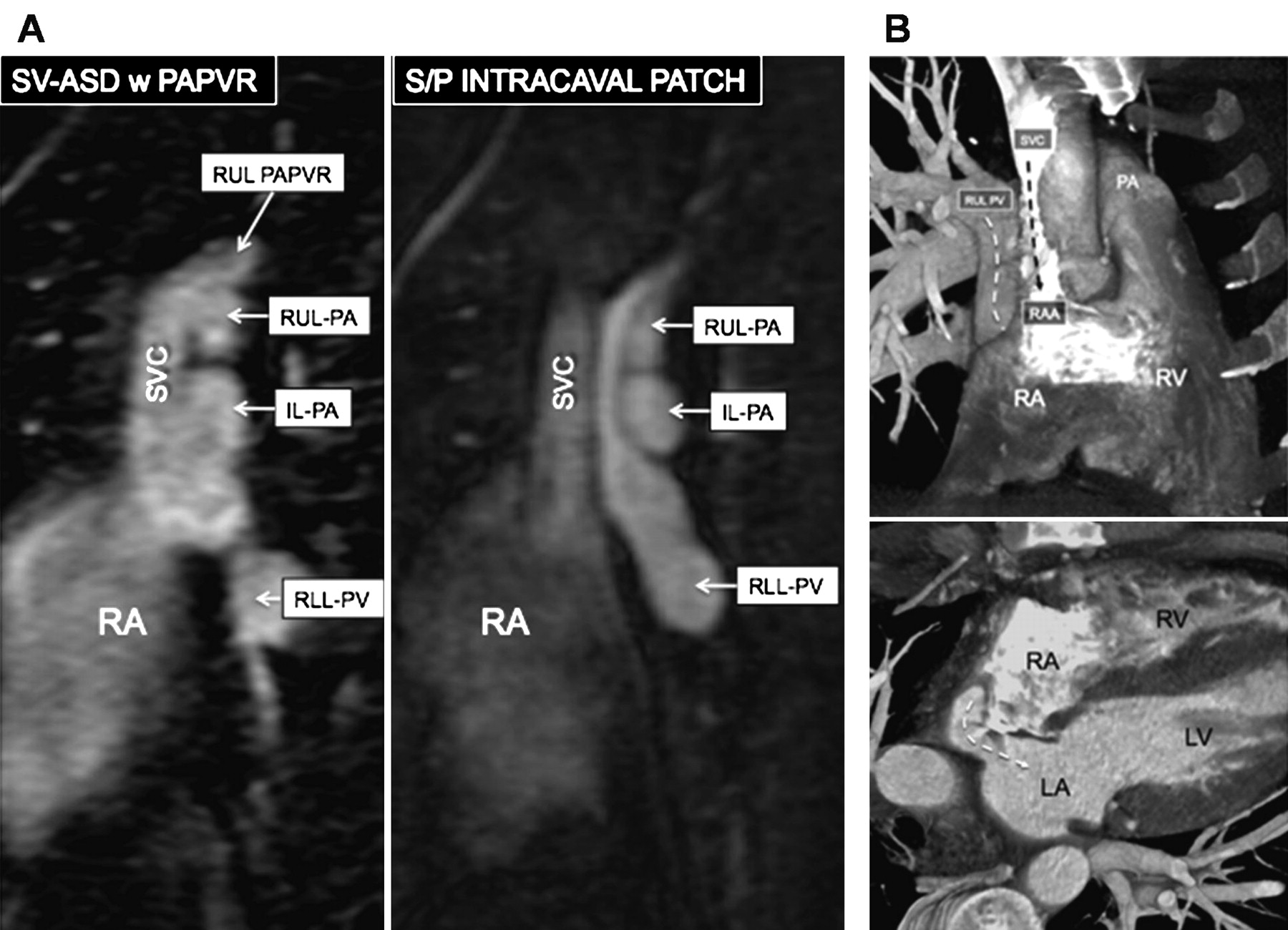
Sinus venosus ASDs, unroofed coronary sinus and ostium primum ASDs should be repaired surgically rather than by a percutaneous technique. Patch closure is usually performed for ostium primum ASDs, unroofed coronary sinus defects, and isolated sinus venosus defects (no associated PAPVR). In patients with SSVDs in whom PAPVR to the SVC is identified, an intracaval baffle (figure 17A) or Warden procedure can be performed (the Warden procedure is the preferred procedure due to a lower complication rate).24 A Warden procedure is an SVC division above the site of the PAPVR with SVC connection to the right atrial appendage and patch baffling of the PAPVR into the left atrium (figure 17B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Sagittal magnetic resonance angiogram images from a 23-year-old man before (left) and after (right) intracaval patch to correct superior sinus venosus atrial septal defect (SV-ASD) with right upper lobe (RUL) partial anomalous pulmonary venous return (PAPVR). (B) Volume rendered images from a cardiac CT in a 34-year-old man after Warden procedure. Upper image demonstrates high density contrast flowing through the superior vena cava (SVC) into the right atrium (RA) through the right atrial appendage (RAA)—superior vena cava anastomosis (black dashed arrow). Note the venous return from the RUL pulmonary vein (PV) has been baffled into the left atrium (LA) (white dashed arrows). IL, intermediate lobe; LV, left ventricle; PA, pulmonary artery; RLL, right lower lobe; RV, right ventricle.
Conclusions
In the majority of the population, the interatrial septum secundum fuses with the septum primum creating a complete physiologic and morphologic separation of the two atria. Deviations from this developmental process can lead to the presence of a number of defects associated with the interatrial septum including a PFO, ostium secundum ASD, ostium primum ASD, sinus venosus and coronary sinus defects. These defects, along with their associated anomalies and sequelae, can be imaged by TTE for initial diagnosis and then confirmed by TOE. In patients in which ultrasound is limited, CT is a desirable alternative due to its rapid acquisition and high spatial resolution.
Imaging of atrial septal defects: key points
Patent foreman ovale (PFO) and atrial septal defects (ASDs) have variable clinical presentations ranging from dyspnoea on exertion to cerebral vascular accidents from paradoxical embolism.
PFO and ASD diagnosis and management requires an understanding of embryologic development patterns and key morphological features of the malformation.
Echocardiography is the primary modality for the diagnosis, morphological assessment, and follow-up of patients with a PFO or ASD.
A PFO is the lack of fusion between the septum primum and the septum secundum within the first few years of postnatal development, which if left untreated may result in right-to-left interatrial shunting and possible paradoxical embolism.
The management of patients with PFOs is still controversial as primary prevention has yet to be established and approved by the FDA.
The four types of ASDs—ostium primum, ostium secundum, sinus venosus, and unroofed coronary sinus ASD—can be differentially detected and diagnosed using a combination of imaging modalities including transthoracic echocardiography (TTE), transoesophageal echocardiography (TOE), and/or CT.
An ostium primum ASD, resulting from the lack of fusion between the septum primum and the endocardial cushions, can be visualised via cardiac CT as an abnormal communication between the right and left atria immediately posterior to the mitral valve annulus.
Ostium secundum ASDs are caused by the incomplete development of the septum secundum or excessive apoptosis of the cephalic portion of the septum primum, and can be effectively visualised as elliptical, circular or irregular shaped defects along the fossa ovalis of the interatrial septum, ideally using real-time three dimensional echocardiography.
Sinus venosus defects occur due to superior vena cava or inferior vena cava malpositioning into the right atrium, or may be observed with TOE or CT as interatrial communication due to deficiencies in the separating wall between the right sided pulmonary veins and the superior vena cava or right atrium.
Unroofed coronary sinus defects result from abnormal cell death during embryologic development and present themselves as a lack of septation between the back wall of the left atrium and the coronary sinus.
Both two dimensional and three dimensional TOE imaging are helpful in determining the suitability of ostium secundum defects for closure, guiding the placement, and assessing postoperative success of percutaneous occluder devices.
Ostium primum, sinus venosus, and unroofed coronary sinus ASDs should be repaired surgically rather than by percutaneous devices often used to repair ostium secundum ASDs.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
We thank CA Rojas for his major role in image acquisition and preparation of the figures.
References
- ↵A detailed review of PFO anatomy, pathology, clinical impact and the therapeutic options available.
- ↵
- ↵A comparative study examining the usefulness of transoesophageal saline contrast echocardiography to conventional transthoracic and transoesophageal colour Doppler echocardiography in the detection of PFO in cryptogenic stroke patients.
- ↵This study indicates the importance of using both saline contrast and colour flow imaging in the diagnosis of PFO as atrial size differentially affects imaging sensitivity.
- ↵A study evaluating the usefulness of multidetector CT in determining anatomical information of the interatrial septum pertinent to the PFO.
- ↵The authors present data obtained via TOE suggesting an association between PFO and stroke resulting from paradoxical embolism in patients over 55 years of age.
- ↵
- ↵
- ↵This study demonstrates the superior sensitivity of the cough test compared to the Valsalva manoeuvre in detecting a PFO during positive contrast TOE.
- ↵
- ↵
- ↵
- ↵This review highlights recent advancements in 3D echocardiography and volumetric image acquisition that allows for real-time 3D modelling. The technology's current use in clinics and growing applicability is also discussed.
- ↵
- ↵The authors of this study confidently conclude that sinus venosus defects result from a deficiency in the wall that normally separates the right pulmonary veins from the superior vena cava and the right atrium resulting in interatrial communication.
- ↵
- ↵This study details the long term postoperative outcome and clinical improvement of patients following sinus venosus ASD repair.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
AMJ and CAR contributed equally to this manuscript.
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The authors have no competing interests.
Provenance and peer review Commissioned; internally peer reviewed.