Article Text

Abstract
Background Cardiac Sarcoidosis (CS) can present with high-grade atrioventricular-block (hgAVB), ventricular arrhythmias or heart failure. The aim of this study was to determine the prognostic impact of a delay in diagnosing CS following presentation with hgAVB.
Methods Consecutive patients, with high grade AVB due to CS referred to our specialist tertiary care hospital between February 2007 to February 2023 were retrospectively reviewed. The median time to diagnosing CS in the study population was used as the cut-off for defining the ‘Early’ cohort. The primary endpoint was a composite of all-cause mortality, cardiac transplantation, ventricular arrhythmic events or heart failure hospitalisation. Secondary endpoints included difference in maintenance prednisolone dose, need for cardiac device upgrade and device complications.
Results A total of 77 CS patients met the inclusion criteria with median time of diagnosing CS as 112 days. Early Group (n=38) was defined as diagnosis of CS within 112 days of presenting with hgAVB. The mean age of the cohort was 54.4 (±10.6) years of whom 64% were male and 81% Caucasian. Patients in the Early Group had a significantly lower median timespan between AVB and first cardiac imaging (echocardiogram, cardiac MRI or FDG-PET scan): 7.5(1.0–35.5) vs 109.5(17.3–357.8) days. Significantly more patients had signs of inflammation on index FDG-PET scan in Late Group (24/27 vs 13/25, p=0.01). After a mean follow up of 54.9 (±45.3) months, the primary endpoint was reached by significantly more patients from the Late cohort (16/39 vs 6/38, p=0.02). On multivariable analysis, late presentation was the only independent predictor of the primary endpoint (HR 6.9 95% CI 1.5–32.2, p=0.01). Patients in Early Group were more likely to have received an Implantable Cardioverter Defibrillator or Cardiac Resynchronisation Therapy-defibrillator device straight after hgAVB (19/38 vs 6/39; p<0.01) and therefore had fewer device upgrades (19/38 vs 30/39, p=0.01) and a trend towards fewer device complications (1 vs 5, p=0.20). The maintenance dose of prednisolone was significantly higher in Late Group [20.70(±.68) mg vs 15.33(±7.87) mg, p=0.02].
Conclusion A later diagnosis of CS led to more overall adverse events, was predictive of clinical outcome, conferred a greater probability of needing an implantable device upgrade and required a higher maintenance steroid dose.
Demographic data in early and late cohort
Devices data in early and late cohorts

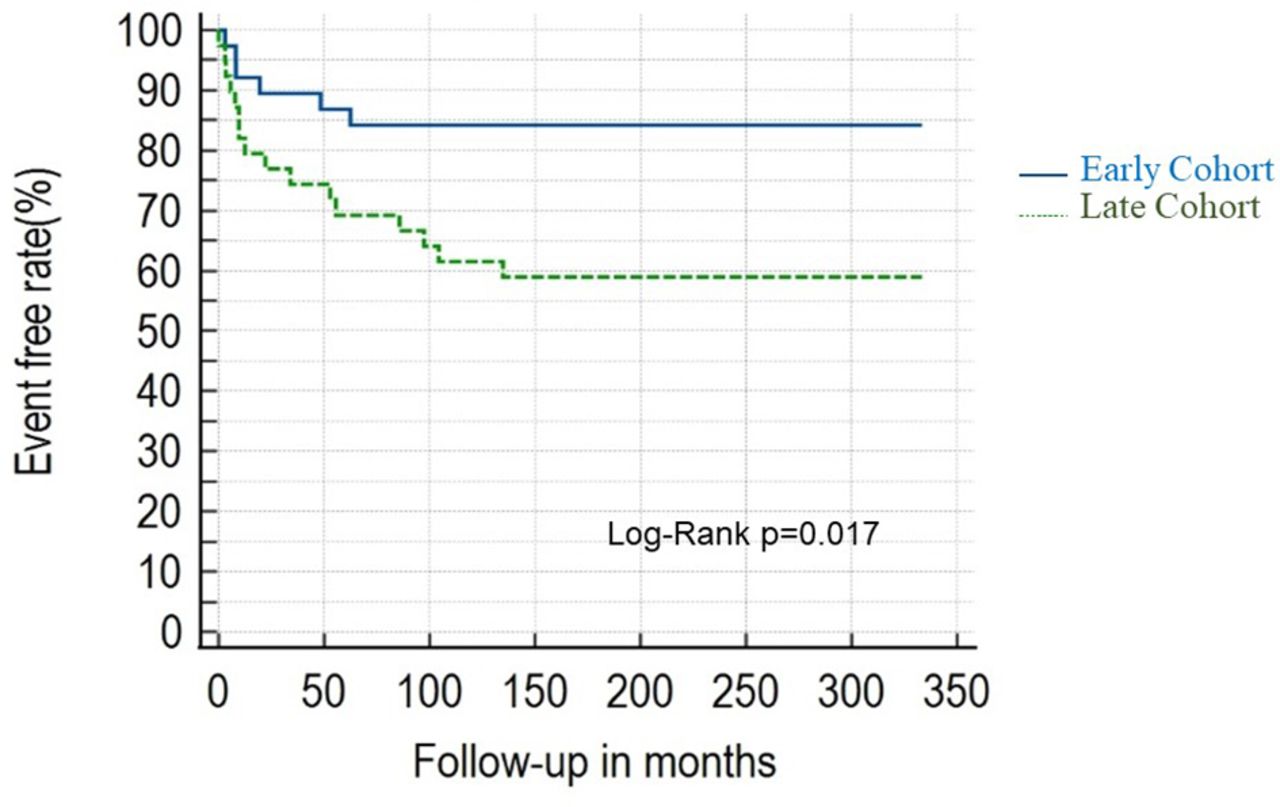
Kaplan-Meier curve for composite end-point in early and late cohorts

{kind=link}
{kind=link}
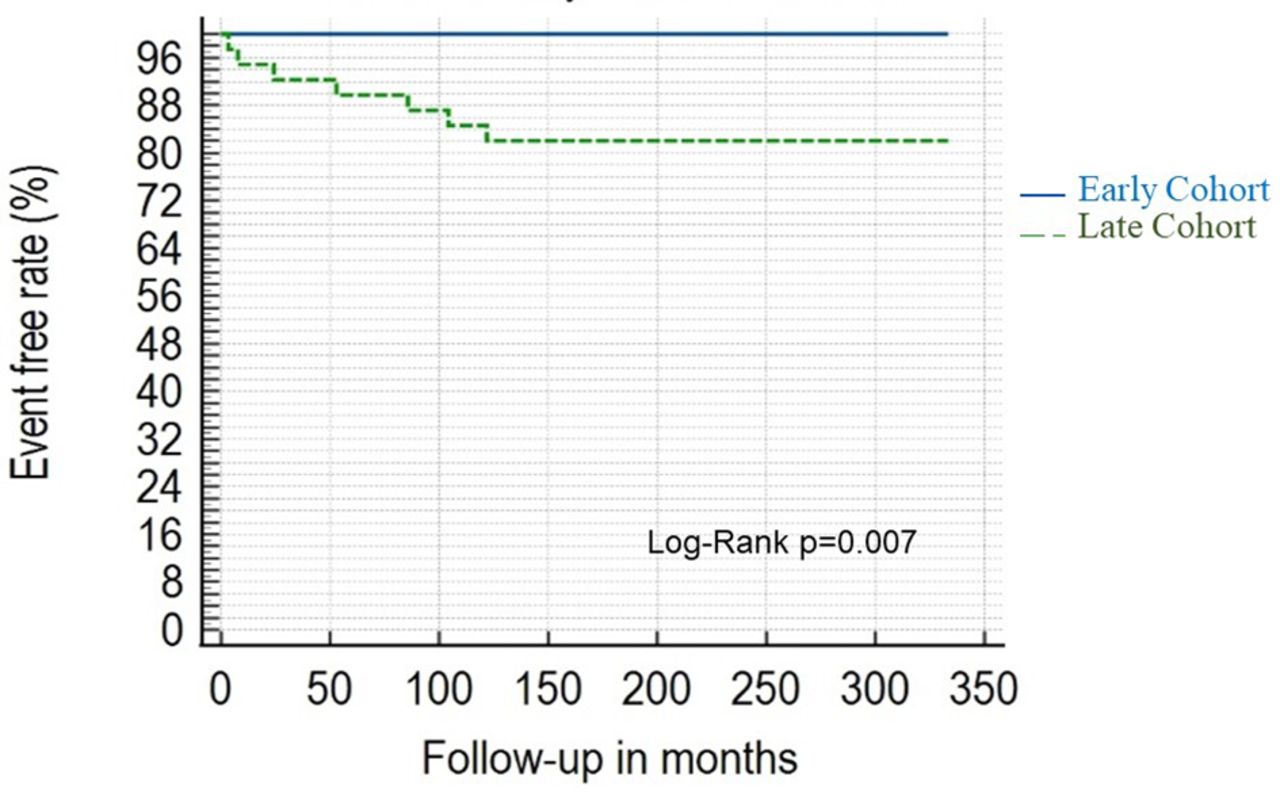
Kaplan-Meier curve for acute heart failure events in early and late cohorts
Conflict of Interest none